Abdominal pain and vomiting in paediatrics
| Disease | Clinical features | Management |
| Appendicitis (all ages) | history of central periumbilical colicky pain that moves to the right iliac fossa over 1 – 2 days and becomes constant. They often vomit (non-bilious) and the vomiting usually starts AFTER the abdominal pain has started. | Bed-side tests: Glucose & MSUU/S abdomen and pelvis Analgesia & keep NBM Fluid resuscitation Surgical review |
| Testicular Torsion | Pain can be referred into the pelvis, abdomen or loins. Examination: a unilateral swollen and tender testicle, with potentially a horizontal (rather than vertical) lie, absent cremasteric reflex, and scrotal erythema | Don’t wait for doppler U/S Urgent Surgical review for ultrasound Exploration within 6 hours to save the testes |
| Malrotation Volvulus (Babies) | Most common in children < 1 year old Symptoms: abdominal pain, bilious vomiting +/- abdominal distension Capillary blood gas show a metabolic acidosis with a raised lactate | Abdominal X-ray, IV fluid and very urgent surgical review |
| Intussusception (Babies and Toddlers) | Common age is 3 – 18 months Usually, after a viral illness. A classic triad of symptoms: episodic screaming with drawing up their legs, vomiting (bilious) and redcurrant jelly stools (but most only have 2/3 of these). Examination: often soft abdomen with tenderness | Need IV fluids, analgesia, NG tube on free drainage, ultrasound examination and urgent surgical referral |
| Necrotising enterocolitis | Commonly in premature infants, particularly those weighing < 1500 gm Symptoms: feeding intolerance, abdominal distension, and bloody diarrhoea at 1 – 2 weeks of age. Other signs & symptoms: abdominal tenderness, abdominal wall erythema, apnoea, lethargy, and bradycardia. | Abdominal x-ray will show dilated loops of bowel and Abdominal ultrasound will show fluid collections Management: Need IV fluids, analgesia, NG tube on free drainage, IV antibiotics & urgent surgical referral |
| Meckel’s diverticulum | Typically, aged < 2 years May present with abdominal pain, and/or painless passage of bright red blood per rectum | Diagnosis by ultrasound abdomen or CT Abdomen scan |
| Mesenteric adenitis | Non- migratory diffuse abdominal pain; history of recent or current URTI, high fever (above 39°C) Abdominal U/S: enlarged mesenteric lymph nodes | Treatment is conservative |
| Hirschsprung’s disease | Most commonly diagnosed in the first year of life Diagnosis: failure to pass meconium in first 36 hours of life strongly suggestive | Abdominal x-ray shows dilated transverse & descending colon. Also, stool may be visible throughout colon. |
| Duodenal atresia | Intolerant of feeding, with nausea and/or bilious vomiting. | Abdominal x-ray demonstrating double bubble gas pattern |
| Pyloric stenosis | Features: Recurrent projectile non-bilious vomiting, typically in a 3- to-6-week-old infant (usually male) and Failure to thrive / weight loss Examination: An olive-shaped mass may be palpable in the right upper abdomen. Diagnosis clinically plus abdominal US | Treatment is with IV fluid and electrolyte replacement, followed by pyloromyotomy (open or laparascopic) |
| Intestinal obstruction | Infant with groin bulge consistent with incarcerated inguinal hernia. The lack of overlying skin oedema and erythema does not rule out strangulation of the small intestine Meconium ileus is an important cause of neonatal intestinal obstruction In small bowel obstruction causing hyperactive bowel sounds (early finding), hypoactive or absent bowel sounds (late finding) | Consider abdominal X-ray Urgent surgical review |
| Ovarian torsion | acute onset of one-sided lower abdominal or pelvic pain; nausea and vomiting common. Tender pelvic mass (adnexal) cervical motion tenderness | Pelvic Ultrasound with colour Doppler can help Always do a beta HCG urine on girls with an acute abdomen |
| Ectopic pregnancy | vaginal bleeding with severe, usually unilateral pelvic pain history of recent early pregnancy or missed last menstrual period | pelvic ultrasound: no intra-uterine pregnancy detected beta HCG urine – positive Diagnostic laparoscopy |
Management of a Child with suspected Gastroenteritis
Viruses account for approximately 70% to 87% of episodes of acute gastroenteritis in children, with Rotavirus and Norovirus being the two most common identifiable causes. Prior to routine rotavirus vaccination, rotavirus was the most common cause of gastroenteritis in the paediatric age group. Currently, norovirus is the most common cause of viral gastroenteritis.
The following children are at increased risk of dehydration:
- Young age (< 1 year of age and especially < 6 months)
- Infants who were of low birth weight
- Those with signs of malnutrition
- Frequent symptoms (> 5 diarrhoeal stools or > 2 vomits within the previous 24 hours)
- Those who are not offered supplementary fluids or stopped breastfeeding prior to presentation
Investigations: –
Consider sending a stool sample for microscopy, culture and sensitivity (MC&S) if:
- The child has recently been abroad to an at-risk area
- The diarrhoea has not improved by day 7
- There is uncertainty regarding the diagnosis
A sample should be sent if:
- Septicaemia is suspected
- There is blood and/or mucus in the stool
- The child is immunocompromised
Blood biochemistry should not be carried out routinely.
Consider measuring laboratory U&Es, venous blood gas and blood glucose if:
- Starting intravenous rehydration
- Hypernatraemic dehydration is suspected
- The child is severely dehydrated / clinically shocked
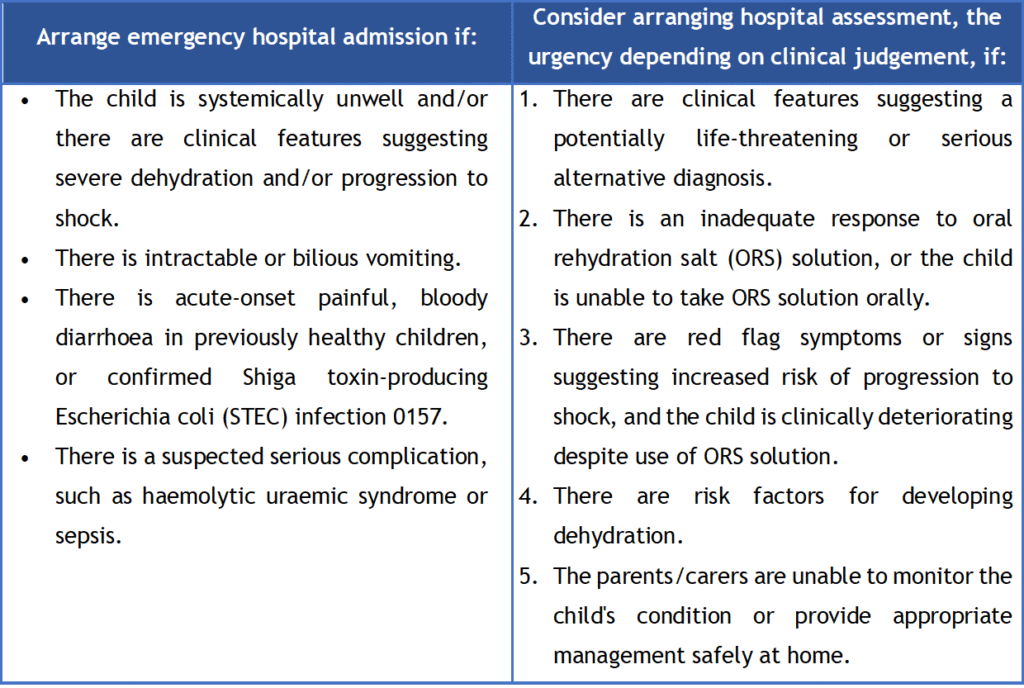
Hospital admission: –
How should I manage a child with gastroenteritis?
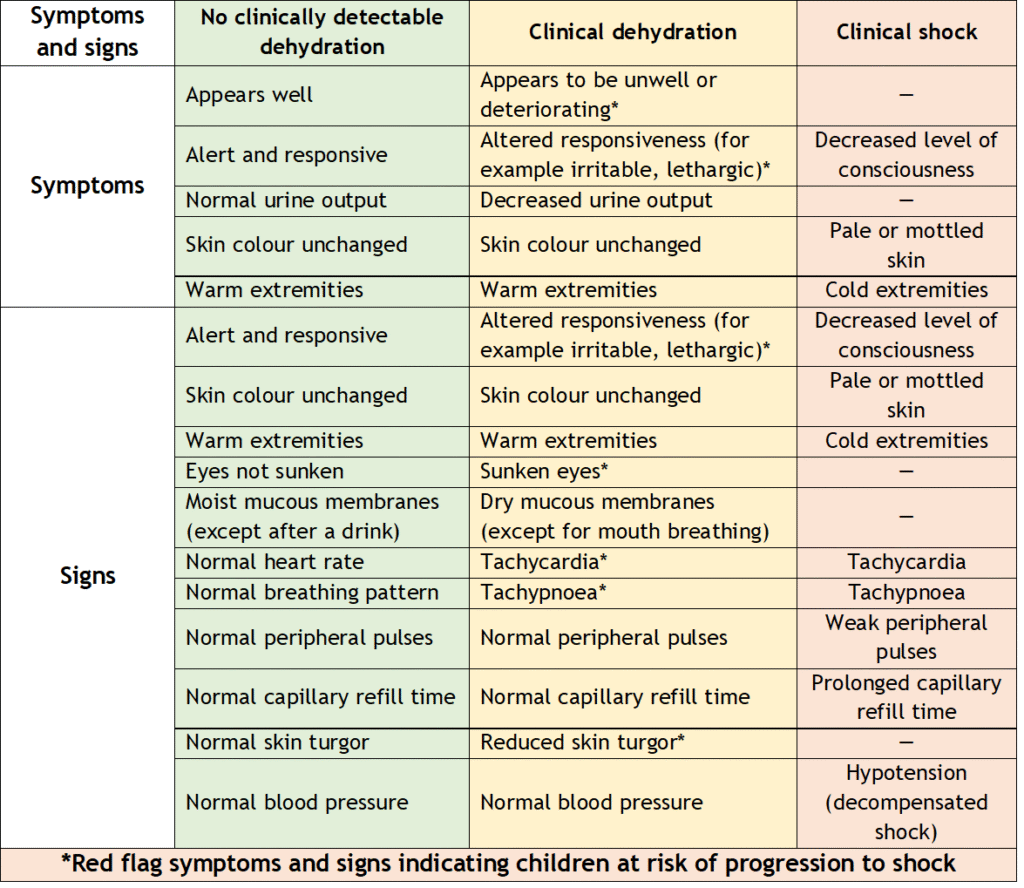
1- Check the symptoms and signs of dehydration and shock.
- < 5% loss = No clinically detectable dehydration (Mild dehydration)
- 5 – 10 % loss = Clinical dehydration (Moderate dehydration)
- > 10 % loss = Severe dehydration +/- shock
2- Start treatment based on severity of dehydration
- Oral rehydration is generally the first-line treatment for all children with acute gastroenteritis who are not clinically shocked.
- Aim for 10 – 20 ml/kg/hr of ORS in frequent small amounts. Replace deficit over 4 hours (NICE guidelines recommend – average 50ml/kg over 4 hrs in mild dehydration and 100 ml/kg over 4 hrs in moderate dehydration).
- Where oral rehydration is not feasible, nasogastric fluid replacement is preferred ahead of IV rehydration.
- Rapid NG replacement: 25ml/kg/hr of ORS over 4 hours
- Standard NG replacement: replace the deficit over the first 6 hours, then give maintenance fluids over next 18 hours.
- This slower regime is preferred in infants <6 months, in the presence of significant comorbidities, or for children with significant abdominal pain.
- IV rehydration is required in cases of shock; dehydration with altered level of consciousness; worsening of dehydration or lack of improvement despite attempts at oral rehydration; persistent vomiting despite appropriate fluid administration; and severe abdominal distension and ileus.
- Resuscitation phase: If the child is clinically shocked, 20ml/kg boluses of 0.9% NaCl should be given. If shock persists after a second, and certainly after a third bolus, consider contacting the paediatric ICU team.
- Rapid IV rehydration with 20ml/kg/hr of 0.9% saline for 2 to 4 hours, followed by oral rehydration is now recommended.
- For IV rehydration, during the initial phase of restoring fluid volume, isotonic fluid (usually 0.9% NaCl) is recommended. Hypotonic solutions are associated with an increased risk of developing hyponatraemia.
- Once fluid volume has been restored, glucose should be added to the saline solution in the maintenance phase of IV rehydration (0.9% NaCl with 5% dextrose).
3- Calculating deficit and maintenance for IV hydration
- Replacing child’s deficit
- Estimate if the child has a 5% or 10% deficit
- Estimated deficit (in ml) is 5% (or 10%) X child’s weight in kg X 10
- Replacing child’s daily maintenance requirements
- 100ml/kg for first 10kg of body weight, then
- 50ml/kg for next 10kg of body weight, then
- 20ml/kg for each subsequent kg of body weight
- Divide this total by 24 to get the hourly maintenance fluid requirements
NG29 Algorithms for IV fluid therapy in children and young people in hospital (nice.org.uk)
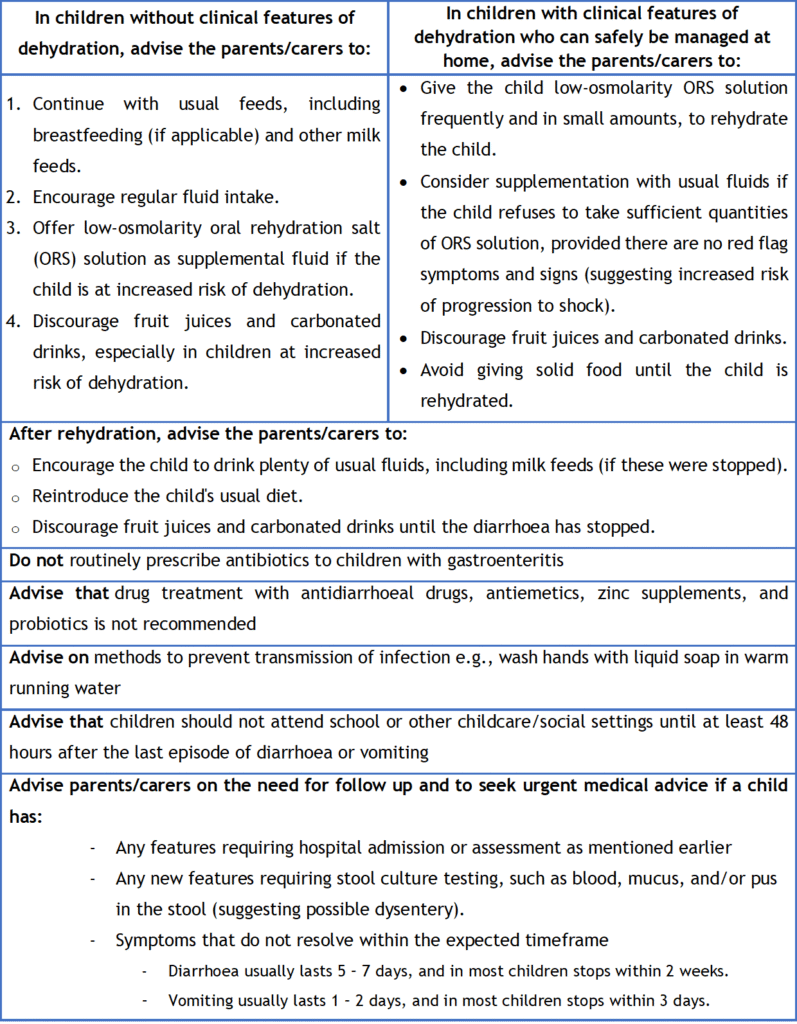
4- Parent/carer advise