Acute coronary syndrome
Definitions:
- Acute myocardial infarction (ST-elevation myocardial infarction (NSTEMI)) is myocardial cell death that occurs because of a prolonged mismatch between perfusion and demand.
- Diagnosed clinically if there is > 1 – 2 mm of ST elevation in 2 contiguous leads on the ECG or new LBBB with a clinical picture consistent with ischemic chest pain.
- Non-ST-elevation myocardial infarction (NSTEMI) is an acute ischaemic event causing myocyte necrosis. Short term mortality is higher with STEMI, but long-term mortality is higher with NSTE-ACS.
- The initial ECG may show ischaemic changes such as ST depression, T-wave changes, or transient ST elevation; however, it may also be normal or show non-specific changes. The patient will have a positive troponin
- Unstable angina is defined as myocardial ischaemia at rest or on minimal exertion in the absence of acute cardiomyocyte injury/necrosis. The initial ECG shows ischaemic changes or non-specific changes as in NSTEMI but with negative troponin.
Clinical Presentation:
- The classic presenting symptom of ACS is chest pain, characteristics of the pain with the highest likelihood for Acute myocardial infarction are radiation of the pain to the right arm or shoulder, or to both arms or shoulders.
- The finding of a third heart sound, hypotension or pulmonary crepitations makes AMI more likely.
Understanding regional blood vessel distribution correlation on ECG
- Inferior STEMI: – characterised by ST elevation in Leads II, III and aVF with Reciprocal ST depressions in aVL +/- lead I. The affected coronary artery is Right coronary artery (RCA)
- RV infarction is suggested if ST elevations are also seen in V1.
- These patients may present with hypotension as the blood pressure is severely preload dependent.
- GTN should be avoided in patients who are presenting with an inferior STEMI
- Diagnosis is confirmed by the presence of ST elevation in the right-sided leads (V3R-V6R)
- AV node is supplied by the RCA. So, inferior STEMI may complicate with bradycardia, 2nd or 3rd degree heart block.
- RV infarction is suggested if ST elevations are also seen in V1.
- Lateral STEMI: – characterised by ST elevation in Leads I, aVL, V5 and V6 associated with Reciprocal ST depressions in leads III and aVF.
- The commonly affected coronary artery is left circumflex (LCx) artery
- Anterior STEMI: – characterised by ST elevation in V1 – V6 as well as the lateral leads I and aVL and Reciprocal ST depressions in III and aVF.
- The affected coronary artery is Left anterior descending artery (LAD).
- Anterior STEMI can be sub-classified to
- Septal = V1-2 (Proximal LAD)
- Anteroseptal = V1-4
- Anterolateral = V3-6, I + aVL
- Extensive anterior = V1-6, I + aVL
- It is associated with the worst outcomes due to involvement of a large amount of muscle within the heart. Patients have higher rates of heart failure, ventricular ectopy (Vfib/VTach) in-hospital, and overall mortality.
- Posterior MI: – characterised by ST-segment depression in leads V1 – V3 with upright T-wave along with signs & symptoms of myocardial ischaemia.
- Confirm with posterior lead ECG (ST-segment elevation ≥ 0.5 mm in V7 – V9).
- The affected coronary artery is RCA or LCx
- Other ischaemic changes: –
- Suspected New Left Bundle Branch Block (LBBB): – Sgarbossa Criteria (highly specific but not sensitive) was used to identify AMI in a patient with LBBB on their ECG.
- Concordant ST elevation ≥ 1 mm in ≥ 1 lead
- Concordant ST depression ≥ 1 mm in ≥ 1 lead of V1-V3
- Proportionally excessive discordant STE in ≥ 1 lead anywhere with ≥ 1 mm STE, as defined by ≥ 25% of the depth of the preceding S-wave
- Wellens syndrome is a pattern of inverted or biphasic T waves in V2-4 (in patients presenting with ischaemic chest pain) that is highly specific for critical stenosis of the left anterior descending artery.
- Type A – Biphasic, with initial positivity and terminal negativity (25% of cases)
- Type B – Deeply and symmetrically inverted (75% of cases)
- Patients may be pain free by the time the ECG is taken and have normally or minimally elevated cardiac enzymes; however, they are at extremely high risk for extensive anterior wall MI within the next 2-3 weeks.
- A pattern of widespread ST depression plus ST elevation in aVR > 1 mm is suggestive of left main coronary artery occlusion.
- A widespread ST depression, seen in leads I, II and V5-6 can be consistent with widespread subendocardial ischaemia.
- Suspected New Left Bundle Branch Block (LBBB): – Sgarbossa Criteria (highly specific but not sensitive) was used to identify AMI in a patient with LBBB on their ECG.
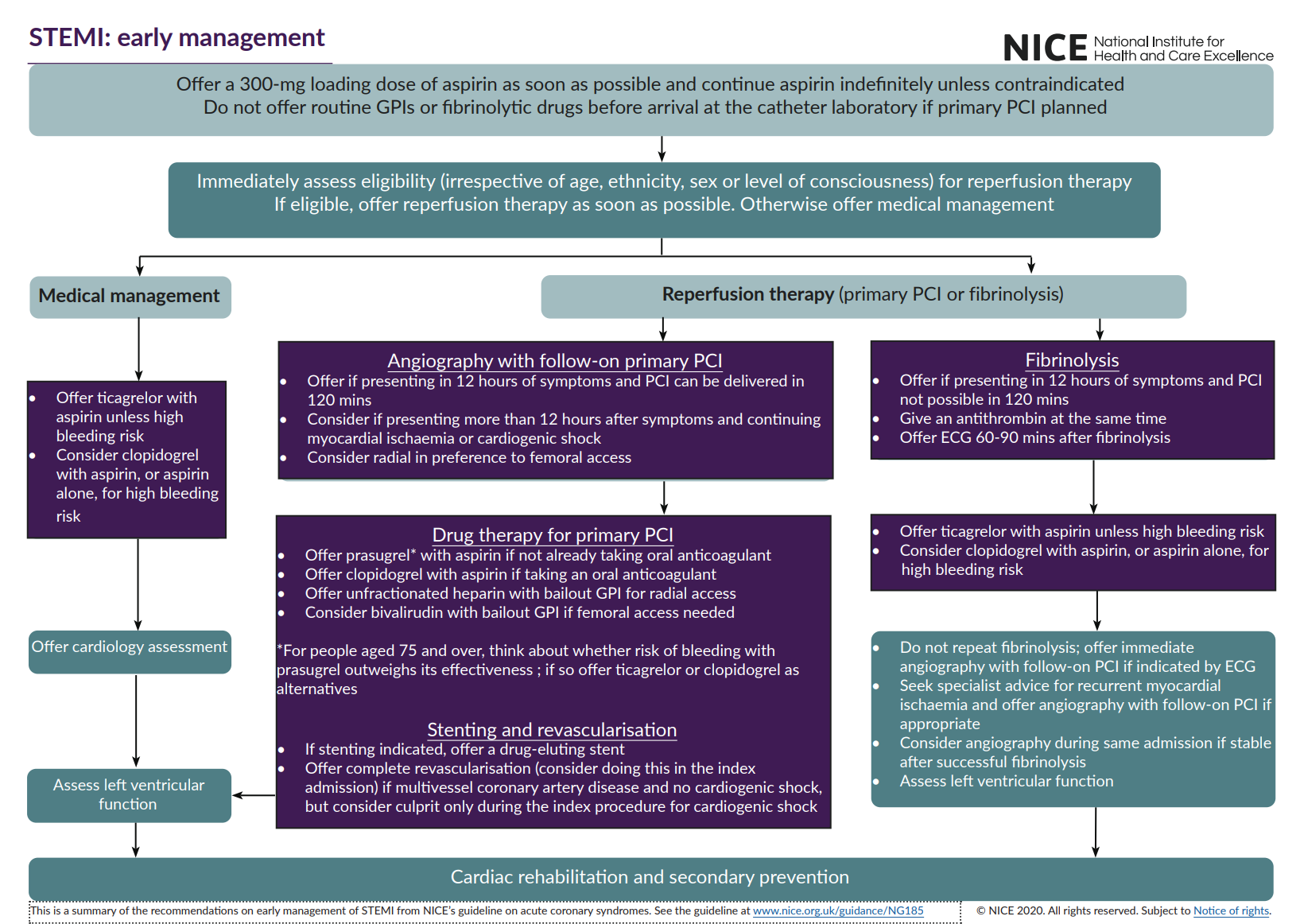
Management of STEMI: –
- Offer a 300 mg loading dose of aspirin as soon as possible.
- Offer opiates, oxygen (if O2 saturation is reduced), GTN and beta-blockers as a part of first aid treatment.
- Immediately assess eligibility (irrespective of age, ethnicity, sex or level of consciousness) for reperfusion therapy then follow the following table: –
Eligible for Angiography with follow-on primary PCI
- Offer if presenting within 12 hours of symptoms & PCI can be delivered in 120 mins
- Consider if presenting more than 12 hours after symptoms and continuing myocardial ischaemia or cardiogenic shock
- Offer prasugrel with aspirin if not already taking oral anticoagulant (think about bleeding risk in people aged ≥ 75 years of age)
- Offer clopidogrel with aspirin if taking an oral anticoagulant
Offer Fibrinolysis only if presenting within 12 hrs of symptoms & PCI not possible in 120 min
- Give an antithrombin e.g., fondaparinux at the same time
- Offer ECG 60 – 90 mins after fibrinolysis
- Offer ticagrelor with aspirin unless high bleeding risk
- Consider clopidogrel with aspirin, or aspirin alone, for high bleeding risk
- Do not repeat fibrinolysis; offer immediate angiography with follow-on PCI if indicated by ECG
Medical management if not eligible for reperfusion therapy
- Offer ticagrelor with aspirin unless high bleeding risk.
- Consider clopidogrel with aspirin, or aspirin alone, for high bleeding risk
Absolute Contraindications to thrombolysis
| Haemorrhagic stroke at any time | Ischaemic stroke within 6 months |
| Recent gastro-intestinal bleeding (within 1 month) | Recent major trauma / head injury (within 3 weeks) |
| Recent major surgery (within 3 weeks) | Aortic dissection |
| Known bleeding disorder | Neurological deficit or CNS neoplasm |
Can thrombolysis be given a patient on warfarin?
In this case, an urgent INR will help in the decision within a reasonable time frame (i.e., within 20 min).
- A sub-therapeutic INR (e.g., < 2.0) would tend to favour administration of thrombolysis, particularly where the potential for benefit is great (e.g., anterior STEMI with an early presentation)
- If the INR is above the therapeutic range (e.g., > 3.0) would contraindicate thrombolysis irrespective of the potential benefit because the risk of ICH is likely to be much higher.
- If the INR is therapeutic (e.g., 2.0 – 3.0) the decision will have to be made based on likely benefit (territory of infarct, timing of presentation) balanced against risk of haemorrhage (advanced age, female gender, low body mass index).
Complications of STEMI and their management:
- Pulmonary oedema – Treatment consists of measures to treat the underlying STEMI (i.e., reperfusion) and specific therapies for left ventricular failure and pulmonary oedema: diuretics, IV nitrates, non-invasive ventilatory support, ACE inhibitors and, where appropriate, tracheal intubation.
- Cardiogenic Shock – Left Ventricular Dysfunction:
- It is characterised by systemic hypoperfusion (tachycardia, reduced systolic blood pressure, cool peripheries and reduced renal output), associated with adequate central venous filling pressures.
- The most effective treatment for cardiogenic shock is early and effective myocardial reperfusion plus specific measures to treat hypotension may be required (e.g., the use of inotropes and/or an intra-aortic balloon pump)
- Right ventricular infarction – It is important to recognise RV infarction because it has implications for management, e.g., Avoidance of nitrates, may require fluid challenge.
- Dressler’s syndrome: – it’s pericarditis post-myocardial infarction or following cardiac surgery.
- Treated by: Aspirin high dose (1 – 2 w) plus Colchicine (3 m)
- Arrythmias include Ventricular or supraventricular arrythmias or Various conduction defects and heart block
- Ventricular aneurysm: seen after large anterior myocardial infarctions.
- ECG features will be new Static ST elevation usually develop 10 – 14 days after an MI.
- Mechanical complications include:
- Mitral regurgitation (the commonest mechanical complication of STEMI). Identified by the presence of clinical signs of sudden haemodynamic deterioration associated with a new murmur
- Ventricular septal rupture: – requires urgent surgery to repair the defect
- Cardiac rupture & tamponade: – associated with sudden haemodynamic deterioration with signs of a cardiac tamponade (hypotension, distended neck veins & muffled heart sounds). Diagnosis is confirmed by echocardiography. Pericardiocentesis may temporarily improve the haemodynamic state, definitive management requires urgent surgery.
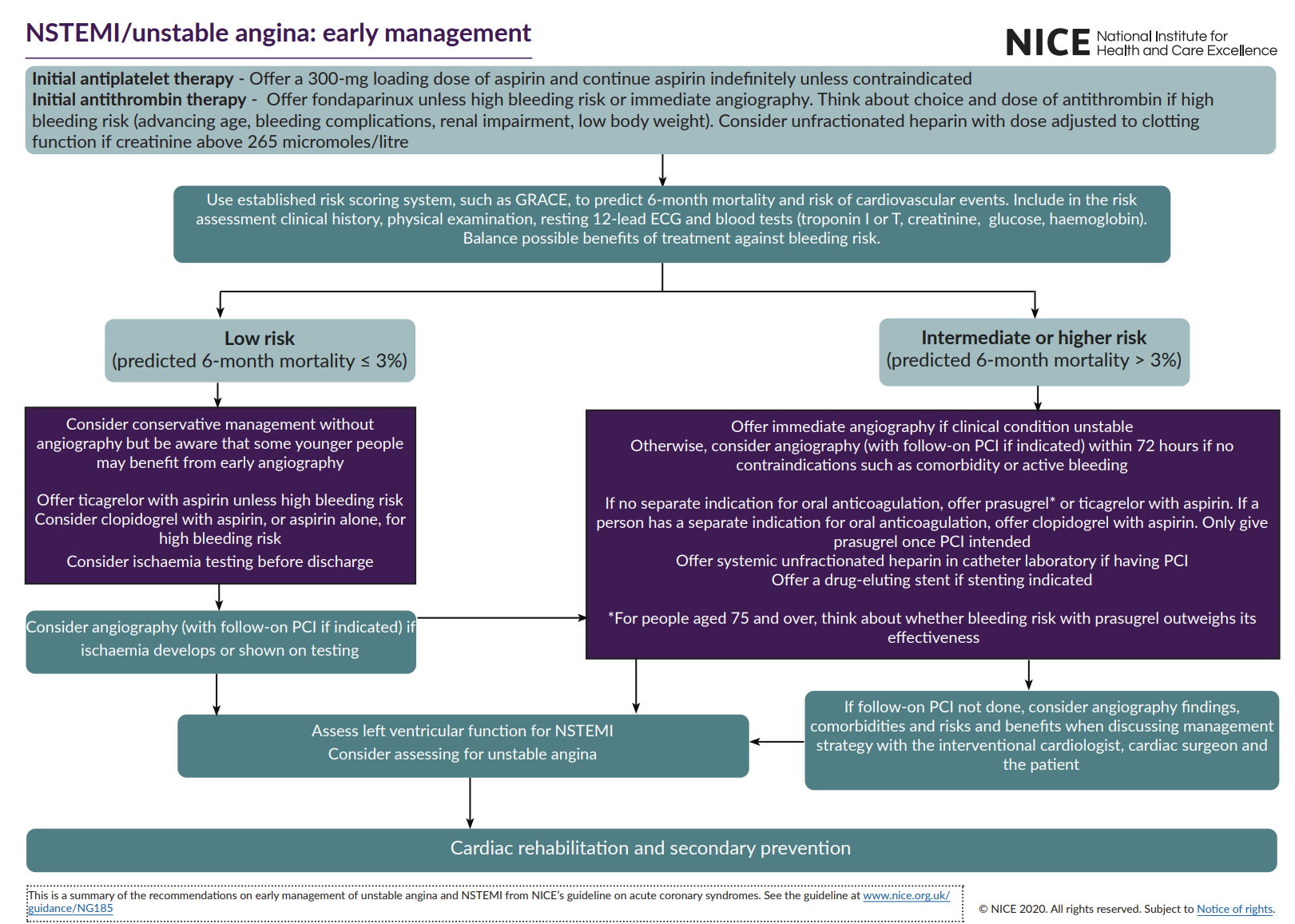
Management of NSTEMI / Unstable angina:
- Initial antiplatelet therapy – Offer a 300-mg loading dose of aspirin and continue aspirin indefinitely unless contraindicated.
- Initial antithrombin therapy – Offer fondaparinux unless high bleeding risk or immediate angiography. Think about choice and dose of antithrombin if high bleeding risk (advancing age, bleeding complications, renal impairment, low body weight). Consider unfractionated heparin with dose adjusted to clotting function if creatinine above 265 micromoles/litre
- Use established risk scoring system, such as GRACE, to predict 6-month mortality and risk of cardiovascular events. Include in the risk assessment clinical history, physical examination, resting 12-lead ECG and blood tests (troponin I or T, creatinine, glucose, haemoglobin).
Mechanism of action of common drugs used in the management of ACS: –
- Aspirin → Cyclooxygenase enzyme inhibitor prevents platelet aggregation and thrombosis.
- Clopidogrel → Anti-platelet agent act by inhibition of the adenosine diphosphate (ADP) pathway
- Prasugrel → is an irreversible, potent platelet receptor antagonist. prasugrel 60 mg
- Ticagrelor → oral anti-platelet agent which is an antagonist to the P2Y12 ADP receptor.
- Fondaparinux → binds to antithrombin-III forming a complex which cause factor Xa inhibition.
- Bivalirudin → Direct Thrombin Inhibitor
- Glycoprotein IIb/IIIa Inhibitors → Glycoprotein IIb/IIIa antibodies & receptor antagonists inhibit the final common pathway of platelet aggregation. All given as IV infusion.
- Abciximab → a chimeric antibody binds irreversibly to the glycoprotein IIb/IIIa Receptors.
- Eptifibatide → a synthetic heptapeptide binds reversibly to the glycoprotein IIb/IIIa receptor.
- Tirofiban → a synthetic small molecule with reversible binding to the glycoprotein IIb/IIIa receptor.
NICE guidelines algorithm