Shortness of breath in paediatrics
Bronchiolitis
Bronchiolitis is a common respiratory illness that primarily affects infants and young children under 2 years of age, with the majority of cases occurring in children under 1 year of age. The illness is characterized by inflammation and obstruction of the small airways in the lungs, often leading to symptoms such as shortness of the breath.
Diagnosis of bronchiolitis
It is typically made based on the clinical presentation and physical examination findings. bronchiolitis typically begins with a coryzal prodrome lasting 1 to 3 days, which includes symptoms such as runny nose, nasal congestion, and mild cough. This is followed by the onset of more severe respiratory symptoms such as persistent cough, tachypnoea (rapid breathing), and chest recession (indrawing of the chest during inspiration). Other common symptoms include wheeze or crackles on chest auscultation and a fever < 39.0 degrees. Some infants may also have poor feeding or apnoea (brief pauses in breathing) during the course of the illness.
If the clinical exam shows bilateral diffuse crackles and wheeze, and there are no focal signs, it is far more likely to be a bronchiolitis than a LRTI. Routine blood gases and CXRs are not recommended. Do a blood gas in patients who require escalation of care to NIV (to some, all kids with bronchiolitis look unwell)
Admit to hospital if the children have any of the following:
- Apnoea (observed or reported)
- If the oxygen saturation is persistently < 92%, for babies < 6 weeks or children of any age with underlying health conditions OR persistently < 90%, for children aged ≥ 6 weeks
- Inadequate oral fluid intake (50% to 75% of usual volume, taking account of risk factors and using clinical judgement)
- persisting severe respiratory distress, for example grunting, marked chest recession, or a respiratory rate of over 70 breaths/minute.
Treatment of bronchiolitis typically includes: –
- Give oxygen supplementation to children with bronchiolitis if the oxygen saturation is
- persistently < 92%, for babies < 6 weeks or children of any age with underlying health conditions
- persistently < 90%, for children aged ≥ 6 weeks
- if you’re struggling to keep the oxygen saturations above 92% on standard oxygen therapy, try HFNC (with appropriate infection control considerations, and senior support).
- Consider CPAP in children with bronchiolitis who have impending respiratory failure
- Do not routinely perform upper airway suctioning in babies or children with bronchiolitis. Saline nasal drops are great immediately prior to a feed, but the effect doesn’t last long.
- NICE recommendation – Consider upper airway suctioning in children who have respiratory distress or feeding difficulties because of upper airway secretions.
- NICE recommendation – Consider upper airway suctioning in children with bronchiolitis presenting with apnoea even if there are no obvious upper airway secretions
- No antibiotics are needed, and although bacterial infection can co-exist, these children generally aren’t given antibiotics. Don’t give bronchodilators, adrenaline nebulisers, hypertonic saline, steroids, Montelukast and most importantly, no trial of inhalers
- Give fluids by NG tube in children with bronchiolitis if taking less than 50% of their usual feeds.
- Give IV fluid in children who do not tolerate NG feeds or have severe respiratory distress
Discharge:
If they are taking > 50% feeds (volume for formula fed babies and total time on the breast for BF babies) AND sats are > 90%.
Notes: –
- Children over the age of 2 are more likely to have bronchospasm, so their wheeze comes on more quickly (hours not days) and is more likely to respond to bronchodilators. In that middle group, aged 1-2 years, if you’re not sure, a trial of inhalers is not evidence based, but may help you make the diagnosis. Make sure that the same person listens before and then again 10-15 minutes after treatment.
- Focal crepitations and lack of wheeze suggest pneumonia rather than bronchiolitis or viral wheeze – if the child’s well, the treatment is the same anyway. If the child requires intubation, you’ll be getting a chest x-ray.
- RSV does live on hands and surfaces for 4 – 7 hours, so keep up all that hand hygiene. Make sure hand washing is emphasised, and see if you can get an extra cleaner to make sure all surfaces are washed regularly.
Viral Wheeze
Viral wheeze is different from bronchiolitis. While bronchiolitis is wet lungs, viral wheeze is bronchospasm. Bronchiolitis is best NOT treated with bronchodilators but viral wheeze MUST be treated with bronchodilators. Viral wheeze is not a benign entity. Children have died from exacerbations of viral wheeze
The treatment of a viral wheeze is all about one thing: β-agonists. Inhaler via spacer is preferable to nebuliser in all situations other than the hypoxic child. Steroids are given for severe episodes but otherwise are not routinely used as the evidence does not support this practice.
Asthma in children
Asthma is rare in the under five year old age group. If asthma is suspected in an under five year old it is usually on the basis of repeated episodes of wheeze that are not related to viral illnesses. Prolonged cough without wheeze is unlikely to be asthma.
Types of asthma exacerbation:
| Acute severe | Life-threatening |
| # SpO₂ <92% # PEF 33–50% best or predicted # Can’t complete sentences in one breath or too breathless to talk or feed # Heart rate > 140/min (1-5 years) or 125/min (> 5 years) # Respiratory rate >40/min (1-5 years) or 30/min (>5 years) | # SpO₂ < 92% # PEF < 33% best or predicted # Exhaustion # Hypotension # Cyanosis # Silent chest # Poor respiratory effort # Confusion |
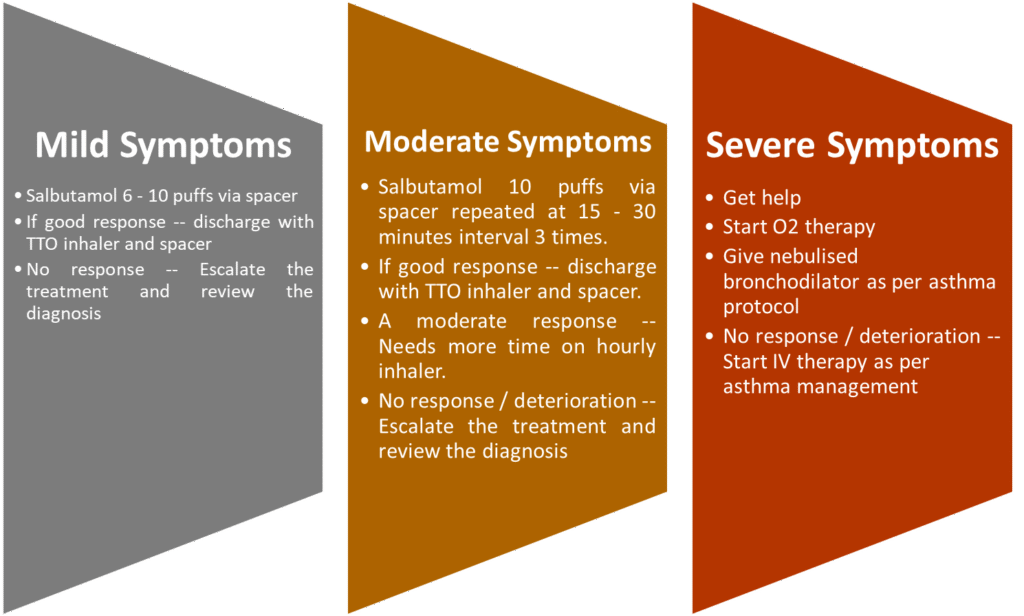
Management of Acute Asthma attack
- Increase β₂ agonist dose by giving one puff every 30–60 seconds, according to response, up to a maximum of ten puffs
- Parents/carers of children with an acute asthma attack at home and symptoms not controlled by up to 10 puffs of salbutamol via a pMDI and spacer, should seek urgent medical attention.
- Children with life-threatening asthma or SpO₂ <94% should receive high-flow oxygen via a tightfitting face mask or nasal cannula at sufficient flow rates to achieve normal saturations of 94–98%.
- Inhaled β₂ agonists are the first-line treatment for acute asthma in children. A pMDI + spacer is the preferred option in children with mild to moderate asthma.
- If symptoms are refractory to initial β₂ agonist treatment, add ipratropium bromide (250 micrograms/dose mixed with the nebulised β₂ agonist solution).
- Consider adding 150 mg magnesium sulphate to each nebulised salbutamol and ipratropium in the first hour in children with a short duration of acute severe asthma symptoms presenting with an SpO₂ <92%.
- Give oral steroids early in the treatment of acute asthma attacks in children. Treatment for up to three days is usually sufficient.
- 10 mg prednisolone for children under 2 years of age.
- 20 mg prednisolone for children aged 2–5 years
- 30–40 mg prednisolone for children > 5 years.
- Those already receiving maintenance steroid tablets should receive 2 mg/kg prednisolone up to a maximum dose of 60 mg.
- Second line treatment – Consider early addition of a single bolus dose of intravenous salbutamol (15 micrograms/ kg over 10 minutes) in a severe asthma attack where the patient has not responded to initial inhaled therapy.
- In children who respond poorly to first-line treatments, consider the addition of intravenous magnesium sulphate as first-line intravenous treatment (40 mg/kg/day).
- Consider aminophylline for children with severe or life-threatening asthma unresponsive to maximal doses of bronchodilators and steroids.
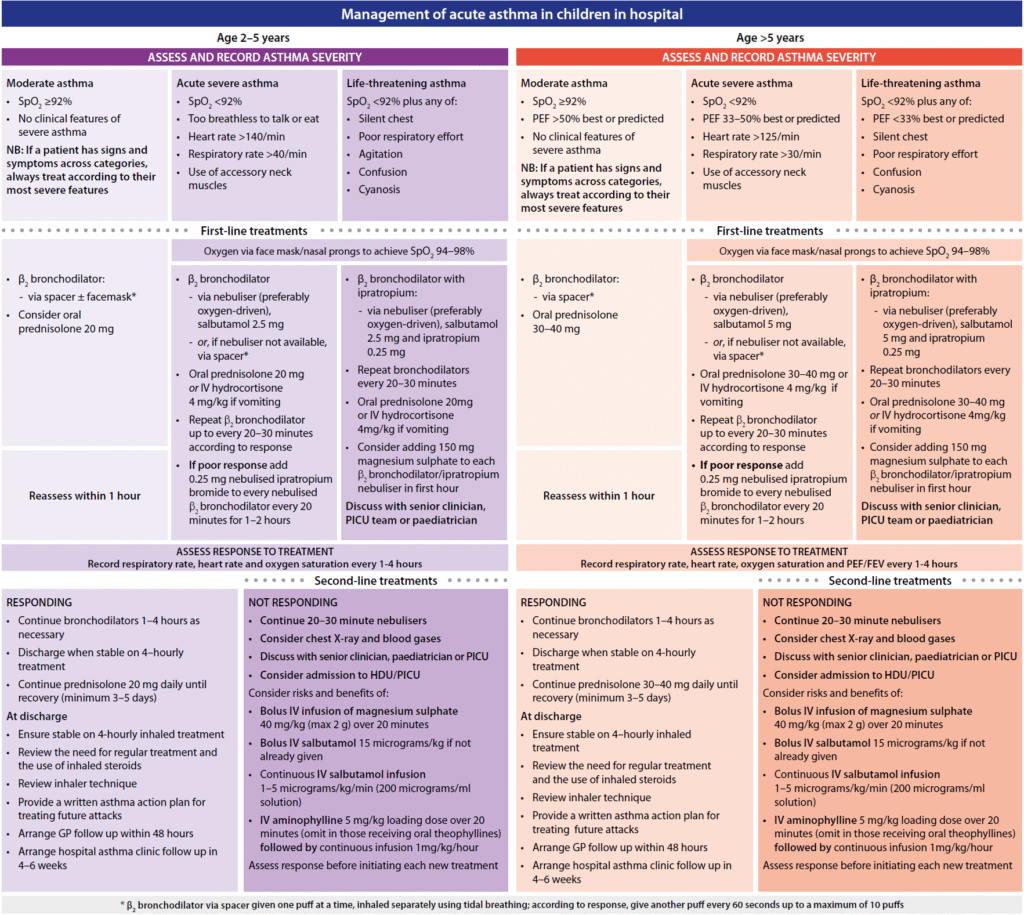
Discharge planning and follow up
- Children can be discharged when stable on 3-4 hourly inhaled bronchodilators that can be continued
- at home. PEF and/or FEV₁ should be >75% of best or predicted and SpO₂ >94%.
- Arrange follow up by primary care services within two working days
- Arrange follow up in a paediatric asthma clinic at about one month after admission
- Arrange referral to a paediatric respiratory specialist if there have been life-threatening features
