Scrotal pain and swelling
Testicular torsion (torsion of spermatic cord)
Definition: Twisting of the spermatic cord, cutting of the blood supply to the testicle, leading to ischaemia
Testicular Torsion can present at any age, most commonly adolescent boys (boys aged between 12 to 18 years are usually at greatest risk), but is less common in the elderly.
Clinical features: –
Testicular torsion should be diagnosed clinically. Clinical providers should have a high index of suspicion maintained in order to identify and provide definitive treatment as quickly as possible.
- Acute, severe unilateral scrotal pain & swelling.
- The pain may radiate to the groin or lower abdominal pain and may be associated with nausea & vomiting.
- May be history of previous episodes of severe, self-limiting pain (torsion & detorsion).
- Severe tenderness to palpation of the affected testicle.
- The testis may have a transverse lie and may be in a higher position (‘high-riding’) than the unaffected testis.
- The cremasteric reflex may be abnormal or absent
- Elevation of the testis does not result in any pain relief (negative Prehn’s sign) as compared to that seen in acute epididymitis
- Scrotal erythema and oedema are late signs
In neonates, extravaginally torsion may present with painless scrotal swelling or mass, with or without acute inflammation.
Investigations: –
if history and physical examination suggest testicular torsion, immediate surgical exploration should take precedence over diagnostic tests.
If the diagnosis is unclear, immediate surgical consultation and exploration may also be warranted.
Management: –
- immediate surgical exploration with intraoperative detorsion and fixation of the testes within 4 – 6 hours of symptom onset.
- Whilst awaiting surgery, it is important to manage symptoms with analgesia and antiemetics.
- Manual detorsion may also be attempted as an adjunct to surgery. This is typically done by rotating the testicle from medial to lateral (clockwise) and usually require at least 360 degrees.
Torsion of appendix testis or appendix epididymis
- May be sudden onset or gradual onset over a few days.
- Typically, self-limiting pain and tenderness over the superior pole of the testis or the epididymis.
- Systemic symptoms and nausea & vomiting are unlikely.
- Cremasteric reflex may be present.
- Blue dot sign – where an inflamed and ischaemic torsed appendage can be seen through the scrotal skin over the superior pole.
Management: – managed conservatively with NSAIDs, ice and support. Pain typically lasts a week and is self-limiting.
Epididymo-orchitis
Definition: Inflammation of the epididymis +/- testes, leading to acute pain or swelling. It may be caused by a sexually transmitted infection or other urinary tract infection spreading along the urinary tract
Clinical features: –
- Acute unilateral scrotal pain and/or swelling +/- fever, dysuria, urethral discharge, or parotid swelling (latter if mumps orchitis).
- Typically, palpable tender swelling of epididymis and/or testis, relieved by elevation of testis (‘Prehn sign’),
- Scrotal skin erythema or hydrocele may be present.
Management: –
- Ensure a urine dipstick test and MSU sample for microscopy & culture have been arranged
- Assess the risk of a sexually transmitted infection (STI), such as chlamydia or gonorrhoea. If suspected STI then advise urgent referral to a local specialist sexual health clinic for STI testing and treatment.
- If Sexually-Transmitted infection suspected (i.e., young patient, new or multiple sexual partners, lack of consistent condom use, known STI contact): Treat empirically with ceftriaxone 1 g IM injection as a single dose, plus oral doxycycline 100 mg twice daily for 10 – 14 days
- If an enteric organism is the most likely cause (older patient, not sexually active, recent instrumentation, urine dipstick positive for leukocytes & nitrites): treat empirically with oral ofloxacin 200 mg twice daily for 14 days, or oral levofloxacin 500 mg once daily for 10 days.
- If a quinolone antibiotic is contraindicated, treat with oral co-amoxiclav 500/125 mg TDS for 10 days.
It is important to safety-net patients discharged home. Advise the patient symptoms should begin to improve within 3 days of starting treatment but may persist for up to 6 weeks. If there is persistence of symptoms patients may require a testicular ultrasound +/- specialist urological or sexual health follow-up to ensure the appropriate treatment was given, that an abscess hasn’t developed and that there isn’t an underlying malignancy.
Other causes for testicular pain and swelling
Fournier gangrene
Fournier’s gangrene is a type I necrotising fasciitis of the perineal and genital region, resulting from synergistic polymicrobial infection.
It is characterized by scrotum pain and redness with rapid progression to gangrene and sloughing of tissue.
As the condition progresses, crepitus, skin necrosis and haemorrhagic bullae may begin to develop
Risk factors: – Diabetes mellitus, excess alcohol intake, poor nutritional state, excess steroid use, haematological malignancies, and recent trauma
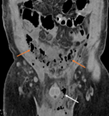
Radiology: – CT pelvis will show soft-tissue gas with possible fascial thickening & fat stranding and will confirm the location & extent of gas distribution in the wounds
Management: – Initial broad spectrum antibiotic therapy (3rd generation cephalosporin, with or without an aminoglycoside for the gram-negative organisms, plus metronidazole for the anaerobes) plus urgent surgical debridement.
Testicular cancer
- Usually unilateral testis enlargement, or change in shape or texture (often painless, may be dull ache or dragging sensation in the scrotum).
- Typically, solid firm mass involving all or part of testis +/- scrotal swelling.
- May be associated supraclavicular lymphadenopathy or abdominal mass (retroperitoneal lymphadenopathy).
- May present with hydrocele or epididymo-orchitis.
Management: – Arrange an urgent urology referral (2-week cancer pathway)
Squamous cell carcinoma of the scrotum
- Gradual onset, often painless raised papule, plaque, ulcer, or non-healing skin lesion on the scrotal wall.
- May be associated inguinal lymphadenopathy.
Management: – Arrange an urgent urology referral (2-week cancer pathway)
Inguinal hernia
- Unilateral inguinal bulge, palpable separate to the testicle; cannot palpate the spermatic cord or inguinal ring above the swollen area.
- May be painful, particularly if incarcerated or strangulated.
- Positive cough impulse and disappear on lying down (if reducible).
Management: – If there is a suspected serious complication ex., strangulation or intestinal obstruction, arrange emergency hospital admission.
Haematocele
- May be sudden or gradual onset, usually pain and tenderness following trauma.
- May transilluminate with a pen torch (to a lesser extent than a hydrocele).
- If it follows acute trauma, arrange emergency hospital admission.
- If it is atraumatic or chronic, arrange an urgent ultrasound of the scrotum and onward urology referral as appropriate.
Epididymal cyst or spermatocele
- The cyst can be palpated separately from the testis, lying posterior and superior to it.
- May transilluminate with a pen torch.
Hydrocele
- painless fluctuant swelling that can have sudden or gradual onset.
- Communicating hydroceles typically fluctuate in size, related to activity or raised intra-abdominal pressure.
- Transilluminates with a pen torch.
- associated with a varicocele, testicular torsion, testicular cancer, or inguinal hernia.
Varicocele
- Gradual onset, usually painless but may be a dull, dragging discomfort in the scrotum when standing.
- The dilated tortuous veins have a ‘bag of worms’ consistency.
- Disappears on lying down; worse on standing, straining, or activity.
Arrange an urgent ultrasound scan of the scrotum, provided a scrotal swelling is not of acute onset, if:
- There is diagnostic uncertainty.
- There is a history of trauma and scrotal pain.
- There are persistent, unexplained testicular symptoms.
- It is not possible to distinguish if the scrotal swelling is testicular or extra-testicular.
- A hydrocele is detected in a person aged 18 – 40 years.
- A haematocele does not follow trauma or is chronic.