Tachyarrhythmias in adults
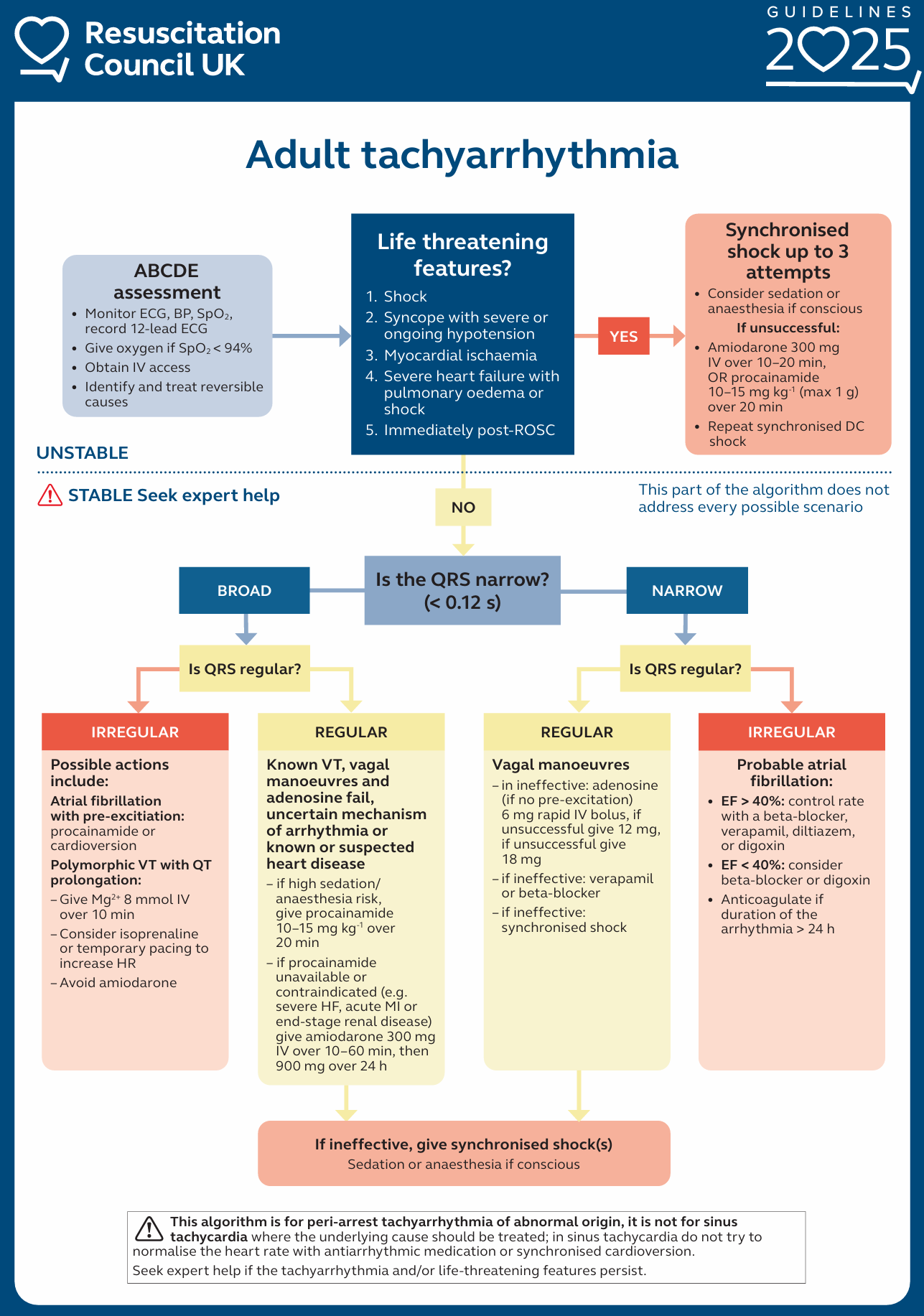
The assessment and treatment of all arrhythmias addresses the condition of the patient (stable versus unstable) and the nature of the arrhythmia. Life-threatening features in an unstable patient include:
- Shock – appreciated as hypotension (e.g., systolic blood pressure < 90 mmHg) and symptoms of increased sympathetic activity and reduced cerebral blood flow.
- Syncope – as a consequence of reduced cerebral blood flow
- Severe heart failure – manifested by pulmonary oedema (failure of the left ventricle) and/or raised jugular venous pressure (failure of the right ventricle)
- Myocardial ischaemia – may present with chest pain (angina) or may occur without pain as an isolated finding on the 12-lead ECG (silent ischaemia).
Electrical cardioversion
It is the preferred treatment for tachyarrhythmia in the unstable patient displaying potentially life-threatening adverse signs.
- Conscious patients require anaesthesia or sedation, before attempting synchronised cardioversion.
- To convert atrial or ventricular tachyarrhythmias, the shock must be synchronised to occur with the R wave of the electrocardiogram (ECG).
- For atrial fibrillation: An initial synchronised shock at maximum defibrillator output rather than an escalating approach is a reasonable strategy based on current data.
- For atrial flutter and paroxysmal supraventricular tachycardia:
- Give an initial shock of 70 – 120 J.
- Give subsequent shocks using stepwise increases in energy.
- For ventricular tachycardia with a pulse:
- Use energy levels of 120-150 J for the initial shock.
- Consider stepwise increases if the first shock fails to achieve sinus rhythm.
If cardioversion fails to restore sinus rhythm and the patient remains unstable (i.e., 3 socks were given but no effect), give amiodarone 300 mg intravenously over 10–20 minutes (or procainamide 10–15 mg kg-1 over 20 minutes) and re-attempt electrical cardioversion (i.e., give the fourth shock). Then, give amiodarone as an infusion of 900 mg over 24 hours.
Pharmacological treatment
If the patient with tachycardia is stable (no life-threatening adverse signs or symptoms) and is not deteriorating, pharmacological treatment may be possible.
- In a patient with haemodynamically stable VT, first-line treatment is conventionally amiodarone (Resus Council UK guidance). However, Amiodarone is poorly effective in the treatment of stable VT, consider electrical cardioversion (as first-line treatment) or Sotalol 100mg (1.5mg/kg) over 5 minutes instead (RCEM learning guidelines).
- Consider amiodarone for acute heart rate control in AF patients with haemodynamic instability and severely reduced left ventricular ejection fraction (LVEF).
- For patients with LVEF < 40 % — consider the smallest dose of beta-blocker to achieve a heart rate less than 110 min-1. Add digoxin if necessary.
Regular broad complex tachycardia: –
- Treat a regular broad complex tachycardia as VT, if the patient is >50 and/or has a history of structural or ischaemic heart disease.
- If there is any doubt whatsoever – treat a regular broad complex tachycardia as VT.
- Following features are suggestive of VT: –
- Evidence of independent atrial activity – dissociated P waves.
- Fusion/Capture beats.
- A bizarre axis.
- QRS >140 msec.
- Concordance of the QRS complexes in the chest leads.