Management of Atrial Fibrillation
Types & Classification: –
Paroxysmal AF – that terminates spontaneously or with intervention within 7 days of onset.
Persistent AF – that is continuously sustained beyond 7 days, including episodes terminated by cardioversion (drugs or electrical cardioversion) after ≥ 7 days
Long-standing / persistent – Continuous AF of >12 months’ duration when decided to adopt a rhythm control strategy.
Permanent AF – that is accepted by the patient & physician, and no further attempts to restore/ maintain sinus rhythm will be undertaken.
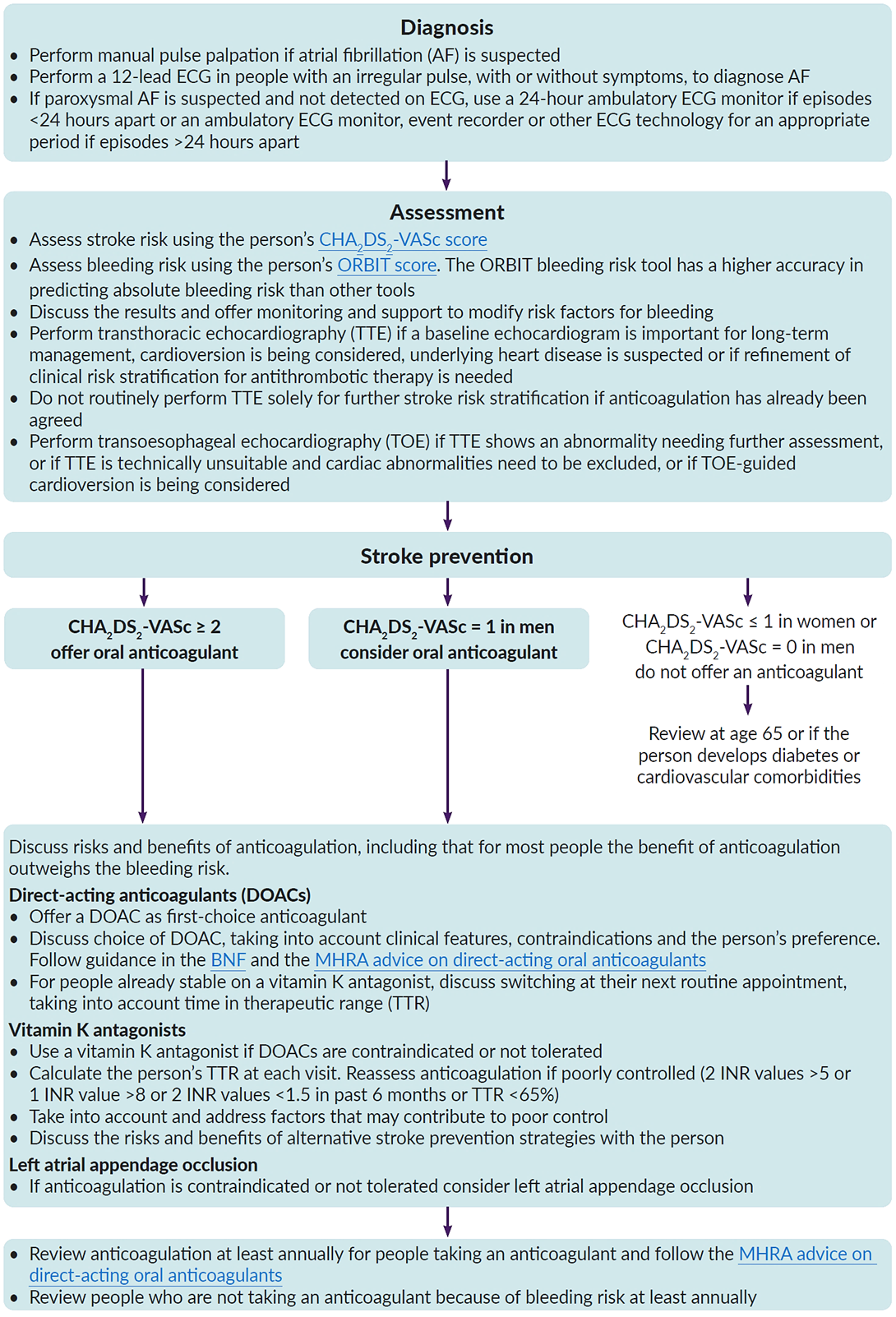
Stroke risk assessment: –
Assess the person’s stroke risk using the CHA2DS2VASc assessment tool: -
- Anticoagulant treatment is indicated if the score is ≥ 2
- Consider Anticoagulant treatment for males with a score of 1
- Do not offer stroke prevention therapy with anticoagulation to people aged < 65 years with atrial fibrillation and no risk factors other than their sex
| C | Congestive heart failure | +1 |
| H | Hypertension or on antihypertensive therapy | +1 |
| A2 | Age 75 years or older | +2 |
| D | Diabetes mellitus | +1 |
| S2 | Stroke: – Previous stroke, TIA, or thromboembolism | +2 |
| V | Vascular disease: – significant CAD, previous MI, PAD, or aortic plaque | +1 |
| A | Age 65 – 74 years | +1 |
| Sc | Sex category (female) | +1 |
bleeding risk should be taking into account by using ORBIT Scoring system: –
- Hb < 13 g/dL for males & < 12 g/dL for females OR haematocrit < 40% for males & < 36% for females
- Age > 74 years
- Bleeding history: – Any history of GI bleeding, intracranial bleeding, or haemorrhagic stroke
- eGFR < 60 mL/min/1.73 m2
- Treatment with antiplatelet agents
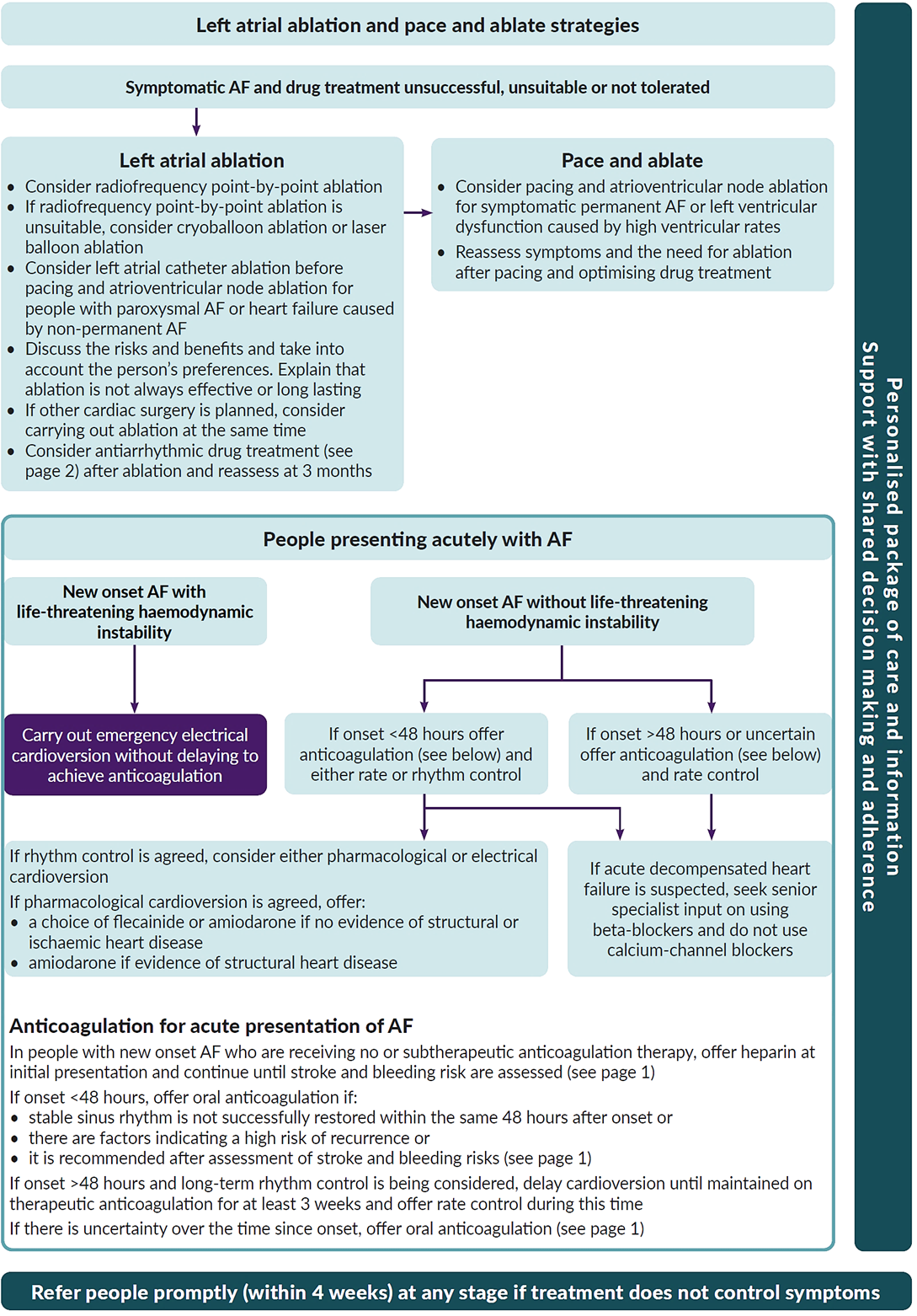
Management of AF: –
| New‑onset atrial fibrillation | ||
| With life‑threatening haemodynamic instability | Without life-threatening haemodynamic instability | |
| ↓ | The onset of the AF is less than 48 hours | The onset of the AF is > 48 hours or uncertain |
| ↓ | ↓ | |
| Carry out emergency electrical cardioversion, without delaying to achieve anticoagulation | Offer either rate or rhythm control | Offer rate control |
| In the absence of contraindications, offer heparin at initial presentation then assess for appropriate antithrombotic therapy based on risk stratification as mentioned before. | ||
A resting HR < 110 bpm should be considered as the initial heart rate target for rate control therapy
In people with atrial fibrillation presenting acutely with suspected concomitant acute decompensated heart failure, seek senior specialist input on the use of beta‑blockers and do not use calcium‑channel blockers. (Beta-blockers and/or digoxin are recommended to control heart rate in AF patients with LVEF<40%)
In people with paroxysmal atrial fibrillation, a ‘pill in the pocket’ strategy should be considered for those who:
- have no history of left ventricular dysfunction, or valvular or IHD and
- have a history of infrequent symptomatic episodes of paroxysmal AF and
- have a SBP > 100 mmHg and a resting heart rate > 70 bpm and
- are able to understand how to, and when to, take the medication.
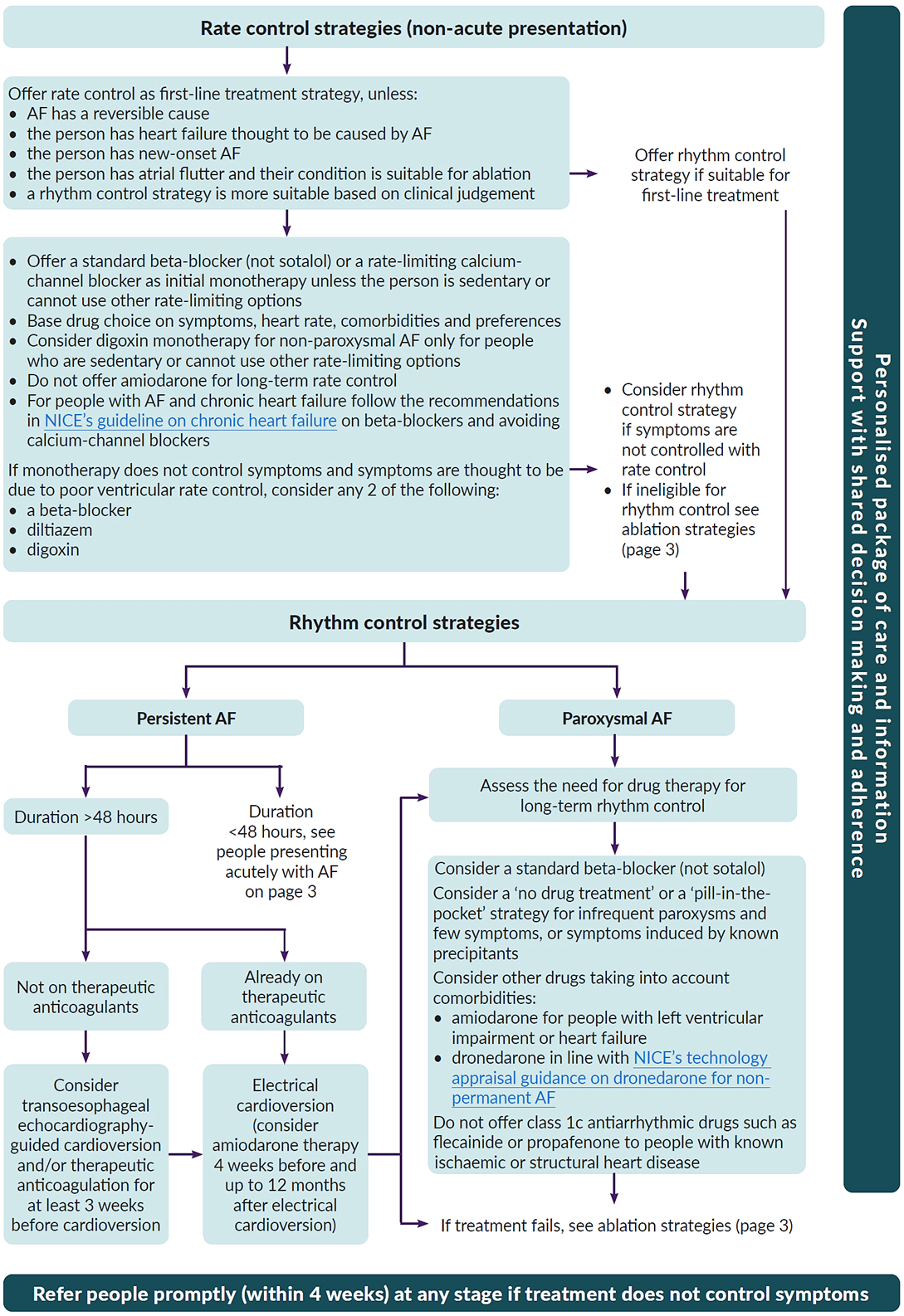
| Rate control | Rhythm control |
|---|---|
| Offer rate control as the first‑line treatment strategy for atrial fibrillation except in people: # whose atrial fibrillation has a reversible cause # who have HF thought to be primarily caused by AF # with new‑onset atrial fibrillation # with A-flutter whose condition is considered suitable for an ablation strategy to restore sinus rhythm # for whom a rhythm‑control strategy would be more suitable based on clinical judgement. | |
| – Offer either a standard beta‑blocker (except sotalol) or a rate‑limiting calcium‑channel blocker (diltiazem or verapamil) as initial rate‑control monotherapy – If monotherapy does not control the person’s symptoms, consider combination therapy with any 2 of beta‑blocker / diltiazem / digoxin – Do not offer amiodarone for long-term rate control. | If pharmacological cardioversion has been agreed for new onset AF, offer: 1- a choice of flecainide or amiodarone to people with no evidence of structural or ischaemic heart disease or 2- Amiodarone to people with evidence of structural heart disease. |
Drugs used in management of AF: –
- Metoprolol tartrate → 2.5 – 5 mg IV bolus; up to 4 doses.
- Oral doses: 25 – 100 mg BD
- Bisoprolol → Oral doses: 1.25 – 20 mg OD.
- Atenolol → Oral doses: 25 – 100 mg OD
- Esmolol → 500 mg/kg IV bolus over 1 min; followed by 50 – 300 mg/kg/min
- Verapamil → 2.5 – 10 mg IV bolus over 5 min.
- Oral doses: 40 mg BD to 480 mg (ER) OD
- Diltiazem → 0.25 mg/kg IV bolus over 5 min, then 5 – 15 mg/h
- Digoxin → 0.5 mg IV bolus (0.75 – 1.5 mg over 24 hours in divided doses)
- Amiodarone → 300 mg IV diluted in 250 mL 5% dextrose over 30 – 60 min (preferably via CV cannula), followed by 900 mg IV over 24 hours diluted in 500 – 1000 mL.
- Oral doses: 200 mg OD after IV loading OR 3 x 200 mg daily over 4 weeks, then 200 mg daily
Novel oral anticoagulants – NOAC – drugs in AF: –
| Drug | Normal dose | Reduced dose and indications |
|---|---|---|
| Dabigatran | 150 mg BD | 110 mg BD in patients with Age ≥ 80 years or Concomitant use of verapamil |
| Rivaroxaban | 20 mg OD | 15 mg OD in patients with CrCl 15 – 49 mL/min |
| Apixaban | 5 mg BD | 2.5 mg BD in patients with at least 2 of 3 criteria: Age ≥ 80 years —— Body weight ≤ 60 kg —— S. Creatinine 1.5 mg/dL (133 mmol/L) |
| Edoxaban | 60 mg OD | 30 mg OD in patients with any of the following criteria: Cr Cl 30 – 50 mL/min Concomitant use of Erythromycin, Cyclosporine, Verapamil, Quinidine, Ketoconazole or Dronedarone |
NICE guidelines algorithms