Arm and elbow injuries
Adult – Humeral neck fracture
The surgical neck fractures occur more than the anatomical neck of the humerus. It may be associated with a greater tuberosity fracture.
A fracture in this area may cause damage to the axillary nerve (didn’t recover despite early surgery).

Neer Classification of Humeral Head Fractures
| Classification | Description | Notes |
| 1 part | Surgical neck, anatomic neck, lesser tuberosity or greater tuberosity | Any fracture pattern with less than 1 cm displacement |
| 2 parts | Surgical neck, anatomic neck, lesser tuberosity or greater tuberosity | Fragments must be displaced by 1 cm |
| 3 parts | Surgical neck and greater tuberosity or surgical neck and lesser tuberosity | Fragments must be displaced by 1 cm |
| 4 parts | Surgical neck, lesser and greater tuberosities | Fragments must be displaced by 1 cm |
Treatment: – Fractures in the elderly without associated joint dislocation and gross rotational deformity can be managed with collar & cuff and be seen in fracture-clinic.
Child – Slipped upper humeral epiphysis
Treatment in children less than 5 years of age is generally conservative.
Treatment in children from 5 to 12 years closed reduction may be required for significantly displaced or angulated fractures in children near the end of growth.
Shaft of humerus fracture
Results from a fall onto an outstretched hand or onto the elbow.
Treatment:
- Check distal pulses, radial nerve and elbow joint.
- Provide analgesia and support the fracture in a POP U-slab or hanging cast POP.
- If displaced, comminuted, angulated or associated with neurovascular complications, then refer for manipulation under anaesthesia (MUA) & internal fixation.

Biceps tendon ruptures
- Rupture of the long head of the biceps tendon (Proximal): bunching of the muscle lower in the arm the so-called Popeye sign. In the majority of cases surgical repair is not indicated.
- Distal biceps ruptures: – the tendon avulses from its insertion on the radial tuberosity usually after a strong contraction. It’s more common in those who have taken anabolic steroids. It needs Repair ASAP. If repair is not carried out patients tend to notice poor supination.

Elbow Injuries
Anterior Humeral Line
- If a line is drawn along the anterior part of the humerus on the lateral radiograph, then it should intersect the middle third of the capitulum.
- Failure to do this indicates that the capitulum has been displaced. There is often posterior displacement in association with supracondylar fractures.

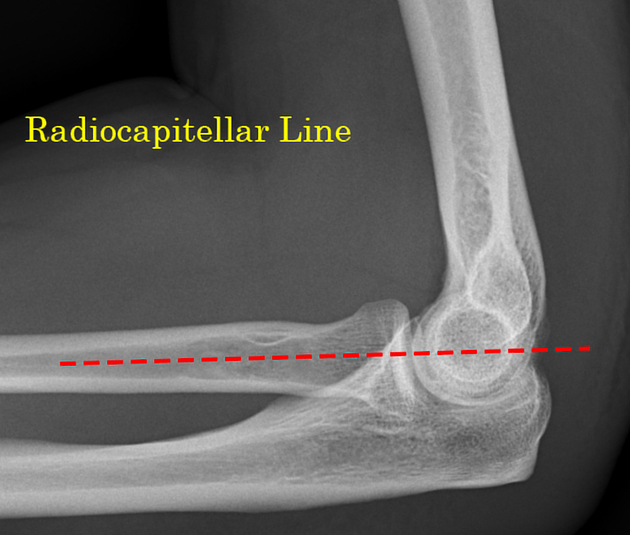
The Radio-Capitellar Line
- A line drawn through the middle of the radius should always bisect the capitulum. This should occur in every direction, no matter which x-ray view is taken.
- Failure to do this suspect dislocation of the radial head and remember that this can sometimes be associated with ulna fractures (Monteggia fracture-dislocation).
Fat Pads
- It is never normal to see a posterior fat pad.
- “The sail sign” due to displaced anterior fat pad in association with a posterior fat pad.
- In the setting of acute trauma, it represents blood in the joint due subtle fracture of head radius. In the non-trauma setting effusion may be due to an inflammatory cause.

Ossification Centres
A well-known helpful pneumonic for this is CRITOL or CRITOE:
| Capitulum | 1 year |
| Radial head | 3 years |
| Internal (medial) epicondyle | 5 years |
| Trochlear | 7 years |
| Olecranon | 9 years |
| Lateral (External) epicondyle | 11 years |
Supracondylar fractures
Typically follow a fall onto an outstretched hand. The peak incidence between 5 – 8 years.
X-rays include presence of fat pads & loss of normal anterior humeral alignment.
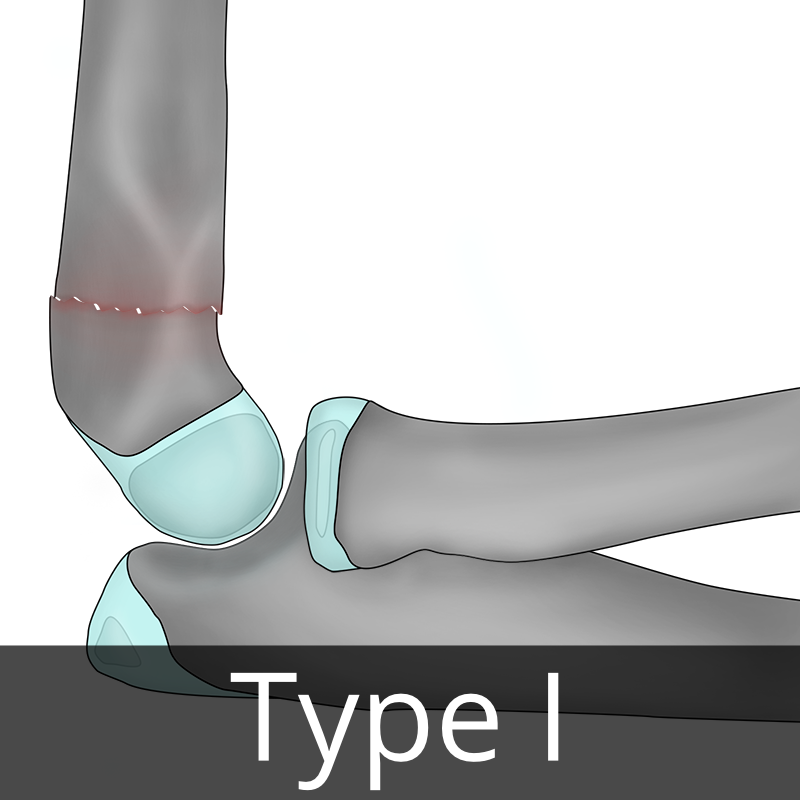
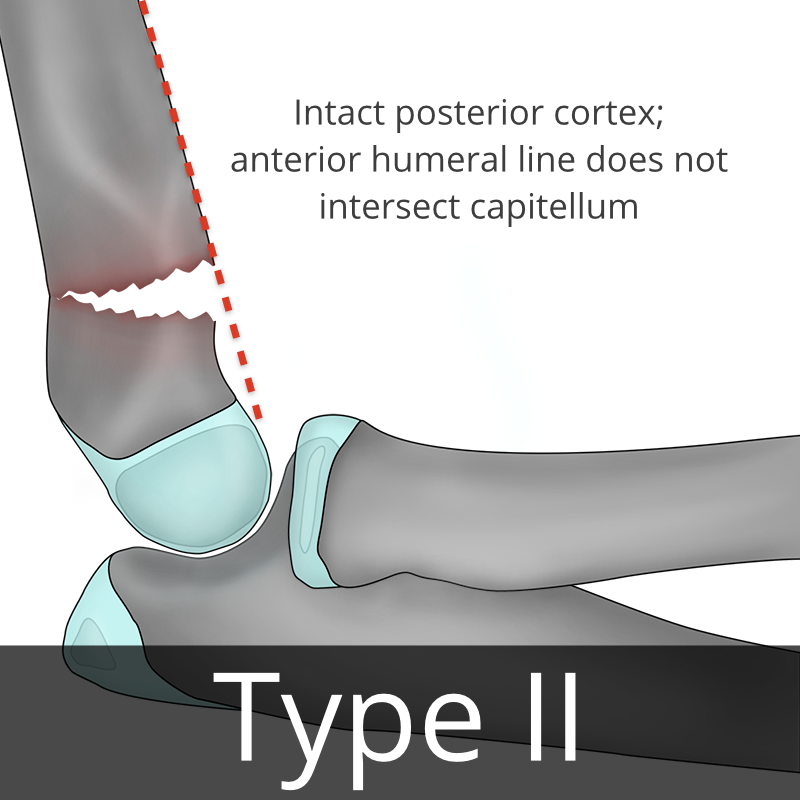
These injuries have been classified by Gartland into 3 types.
- Type 1 is an un-displaced fracture (accounts for 25% of injuries).
- Type 2 represents a fracture with posterior displacement but with an intact posterior cortex.
- Type 3 injury has posterior displacement with complete cortical disruption.
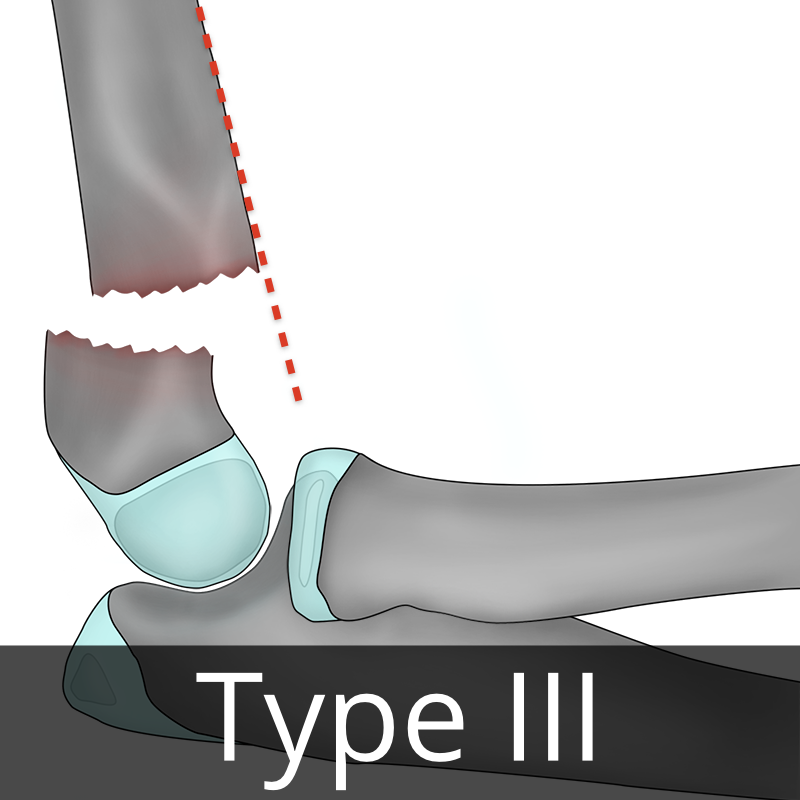
Case courtesy of Andrew Murphy, Radiopaedia.org. From the case rID: 97447
Treatment
- Analgesia and neurovascular assessment.
- Un-displaced fractures may be treated with a collar and cuff and can be followed up in fracture clinic. If there is significant pain, a back slab may be a better option.
- Displaced fractures should all be referred for manipulation, urgently if circulation is compromised.
Complications include:
- Cubitus varus (gun stock deformity)
- Malunion and stiffness
- Myositis ossificans
- Nerve injury (most commonly median nerve)
- Brachial artery (due to stretch and posterior displacement)
- Volkmann’s ischaemic contracture (due to compartment swelling)
Lateral epicondyle epiphyseal injury
This is the 2nd most common elbow fracture seen in children, usually between age of 4 – 10 years.
It results from a varus force applied through the extended elbow, normally due to a fall on an outstretched hand.
It is commonly displaced by the action of the forearm extensors.
Displaced fractures often need reduction whereas un-displaced fractures can be managed in a back-slab with orthopaedic follow up.

Medial epicondyle avulsion injury
These injuries tend to occur in adolescents due to valgus stress during a fall on an outstretched hand.
There may be associated ulna nerve damage & elbow dislocation.
Un-displaced avulsions can be managed conservatively while displaced fragments should be referred for reduction.

Elbow dislocation
Caused by a fall onto the outstretched hand.
Clinical examination: –
- The triangular relationship of the epicondyles and olecranon will be disrupted.
- Posterior dislocation is more common.
- Risk of damage to the brachial artery or median and ulnar nerves.
- Associated epicondylar fractures and fractures of the lateral condyle may occur in children.
Treatment
- Analgesia, Procedural sedation (with full monitoring) is likely to be required.
- Reduction should be immediately followed by a further neurovascular assessment.
- Immobilise in a back-slab in 90 of flexion. Confirm the reduction by repeat x-ray.
- Outpatient orthopaedic review should subsequently be arranged.

Radial head fractures
Caused by a fall onto an outstretched wrist or direct trauma.
Clinical examination: pain may only be evident with palpation of the radial head during passive forearm pronation. Elbow extension is usually restricted.
Radiography may reveal the fracture or merely the presence of a joint effusion.
Treatment
- Greater than 20 of angulation in the adult requires reduction.
- Un-displaced fractures can be managed with a collar & cuff sling and fracture clinic follow-up.
- Comminuted or displaced fractures may require MAU or internal fixation.

Radial neck fractures are seen more commonly in children and are managed similar to radial head fractures. Greater than 20 degrees of angulation in the adult requires reduction.
Olecranon fractures
Caused by a fall onto the point of the elbow or onto a semi-flexed outstretched forearm.
Examination will reveal swelling and tenderness over the posterior aspect of the elbow. Radiography will confirm the diagnosis and also reveal any displacement due to the pull of the triceps tendon.
Un-displaced fractures – treat with a back-slab in 90° flexion of elbow and fracture clinic follow-up.
Displaced fractures (> 2mm) or comminuted fractures may require operative fixation.

Monteggia fracture-dislocation
Defined as: ulnar fracture associated with dislocation of the radial head. (Manchester United Discharged Ronaldo)
Caused by: a direct blow to the ulna or forced pronation.
Suspect in X-ray: if there is fracture ulna with disruption of the Radio-Capitellar Line
Treatment: open reduction & internal fixation in adult. Children can be treated with Closed reduction.

Galeazzi fracture-dislocation
Defined as a fracture of the radius associated with dislocation of the distal radio-ulnar joint at the wrist
Treatment: analgesia & immobilization in a temporary POP back-slab. Refer for ORIF.
Pulled elbow
Caused by: traction on the arm of a child between 1 – 5 years, although this is not always the case.
Results from: subluxation of the radial head from its position encircled by the annular ligament.
Elbow x-ray is normal, and it is not necessary prior to attempted manipulation.
Reduction method: achieved by applying pressure over the radial head then fully pronating the forearm followed by flexing the elbow to 90° (Click will be heard & the child will begin using the arm a short time later).
Other soft tissue injuries
| Olecranon bursitis | # It may be acute from direct trauma or chronic and can be associated with crystal arthropathy or inflammatory arthritis. Septic bursitis is most commonly due to Staphylococcus aureus infection. # Examination: localised swelling & tenderness +/- erythema over the posterior aspect of the elbow. # Patients with septic bursitis may be systemically unwell with fever, cellulitis & axillary lymphadenopathy. # Blood tests: may reveal an elevated ESR, CRP and white cell count. Septic or crystal-induced bursitis can be confirmed with bursal aspiration and subsequent microscopy and Gram stain. # Management: Rest in broad arm sling & analgesia. Septic bursitis requires antibiotics as per local policy. |
| Lateral epicondylitis (Tennis elbow) | * An overuse of the forearm extensor tendons. * The patient complains of a diffuse ache located over the lateral aspect of the elbow. * Management: relative rest, ice therapy and analgesia. Steroids injection & physiotherapy may help. |
| Medial epicondylitis (Golfers’ elbow) | – An overuse injury of the forearm flexor tendons – pain over the medial aspect of the elbow. – In 20% of cases ulnar nerve symptoms may be present, specifically paraesthesia in an ulnar nerve distribution. – Management: relative rest, ice therapy and analgesia. Steroids injection & physiotherapy may help. |