Acute loss of vision
Common causes of acute vision loss: –
- Amaurosis fugax – Sudden onset of monocular vision loss, with complete resolution. It is usually embolic or thrombotic; can occur secondary to hypoperfusion states, hyperviscosity or vasospasm
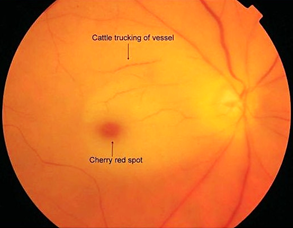
- Central retinal artery occlusion – this would present with sudden painless loss of vision and classically a ‘cherry red spot’ on fundoscopy.
- Central retinal vein occlusion – acute monocular loss of portion of visual field.
- Optic neuritis – the triad of unilateral acute vision loss (or central scotoma), eye pain worse on movement and impaired colour vision suggests a diagnosis of optic neuritis.
- Retinal detachment – this would present with flashes, floaters, sudden-onset painless vision loss and the patient may describe a ‘dark shadow or curtain’ obscuring their vision
- Giant cell arteritis – in patients > 55 years old, usually present as New-onset headache, Temporal artery abnormality, Intermittent jaw claudication and Visual disturbances such as loss of vision, diplopia, or changes to colour vision.
- Orbital apex syndrome – This is a compartment syndrome usually caused by retro-bulbar haemorrhage or orbital cellulitis.
- Vitreous hemorrhage – caused by diabetic retinopathy or trauma. characterised by a sudden onset of floaters followed by diffuse vision loss; monocular; usually painless.
- Ocular migraine – characterised by scintillating scotoma, within 1 hour of migrainous headache.
- Idiopathic intracranial hypertension (IIH) – It can present with headache plus transient binocular vision loss on bending down and on coughing
- Hypertensive retinopathy – fundoscopy may show AV nipping, flame haemorrhages and hard exudates. Papilloedema may be present in severe hypertensive retinopathy and headache and visual disturbance can be present since this condition causes neurological symptoms.
- Pituitary Tumour – sudden or sub-acute onset of central or peripheral vision loss; painless (likely bitemporal hemianopia)
Central retinal artery occlusion
The pupil of affected is poorly reactive to light reflex but with normal consensual light reflex.
Characterised by: –
- Reduced visual acuity and abnormal asymmetrical red reflex
- On fundoscopy: – the retina will appear diffusely pale with cherry red spot in the macula.
Treatment: –
- Refer to ophthalmologist
- Immediate digital ocular massage to induce oscillations of intraocular pressure and dislodge the offending thrombus.
- Intraocular pressure reduction by re-breathe CO2, timolol eye drops and/or Acetazolamide 500mg IV.
- Supplemental oxygen.
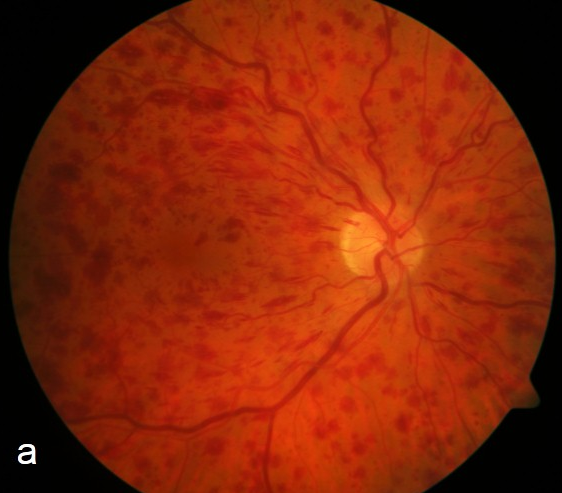
Central retinal vein occlusion
Retinal vein occlusion (RVO) is an interruption of the normal venous drainage from the retinal tissue.
RVO frequently presents as sudden, painless, unilateral vision loss. Most affected patients are aged >65 years.
Characteristically, in the retina proximal to the occlusion, the affected venous system is tortuous and dilated, and there are several intra-retinal haemorrhages and retinal oedema (stormy sunset appearance).
Treatment: – Refer to ophthalmologist for photocoagulation
Orbital apex syndrome
This is a compartment syndrome usually caused by retro-bulbar haemorrhage or orbital cellulitis. The rising pressure results in ischaemia to the sensitive neurological tissues of the optic nerve and retina and can be devastating to sight in minutes. So, Early recognition and intervention are vital to optimising visual outcome.
Risk factor such as facial trauma, a coagulation disorder or recent infection.
Symptoms may include: Severe eye pain, Profound vision loss, Diplopia
Signs may include:
- Proptosis – fullness of the left upper lid denoting proptosis
- Restricted eye movements
- Poor visual acuity
- High intraocular pressure by tonometry
- Subconjunctival haemorrhage
- Swollen and bruised lids

Management: –
If orbital apex syndrome is likely, remember “Time is Vision“. Lateral canthotomy and cantholysis is a quick and safe procedure with minimal risks to the patient and huge potential benefits. The only contraindication would be an open globe, which would warrant discussion with ophthalmology.