Abdominal Trauma
The abdominal contents can be divided into:
- The intra-abdominal structures
- Retroperitoneal structures
- The pelvic structures
A useful mnemonic to remember which organs are retroperitoneal is: SAD PUCKER
S: suprarenal (adrenal) gland
A: aorta/IVC
D: duodenum (second and third part)
P: pancreas (except tail)
U: ureters
C: colon (ascending and descending)
K: kidneys
E: (o)oesophagus
R: rectum
Abdominal regions and organs potentially injured
| Region | Organs potentially injured |
| Lower chest | Liver, spleen, diaphragm, stomach |
| Anterior abdomen | Liver, spleen, colon, bladder, stomach, pancreas, transverse colon, ileum, jejunum |
| Flank | Kidneys, ureters, ascending and descending colon |
| Posterior abdomen | Great vessels, duodenum, pancreas, spinal cord |
Penetrating Abdominal Trauma
Do not remove any object from the wound, such as a knife, as this may be tamponading underlying vessels.
Patients with penetrating injury, even with normal vital signs, should be assessed by a senior surgeon & all patients should be admitted for observation even if no further investigation is initially required.
Most commonly involved abdominal structures in stab wounds are liver (40%), small bowel (30%), diaphragm (20%), and colon (15%).
Blunt Abdominal Trauma
It has greater mortality than penetrating as there is often injury to multiple organ systems.
The most commonly injured intraperitoneal organs in blunt trauma are spleen (commonest) then liver then small bowel.
Other common injuries include mesenteric tears, bowel perforation, and abdominal aorta injuries.
Proton pump inhibitors will delay the onset of symptoms of peritonism in gastric perforation by reducing the acidity of the contaminating fluid.
Liver injury
Liver injuries account for 15-20% of intra-abdominal organ injuries but up to 50% of mortality, and 45% have associated splenic injury.
Conservative management is appropriate in 80% of cases, with surgical intervention reserved for ongoing and uncontrolled bleeding.
If hepatic or splenic injuries are detected on CT, the source of any ongoing bleeding can be detected through angiography. Through interventional radiology it can be possible to embolise the bleeding vessel and avoid the need for surgical intervention.

{kind=link}
Splenic injury
The spleen contains approximately one unit of blood at any time.
It is graded according to CT findings and treatment is guided by grade:
| Grade 1 | Minor subcapsular tear or haematoma – managed conservatively. |
| Grade 2 | Parenchymal injury not extending to the hilum – managed conservatively. |
| Grade 3 | Major parenchymal injury involving vessels and hilum. |
| Grade 4 | Shattered spleen |

{kind=link}
Pancreas
* Injury to the pancreas may cause pancreatitis, which may develop over days.
* Blunt pancreatic injury may not be immediately recognised. It is relatively uncommon, occurring in around 10% of blunt abdominal injuries but it is rarely an isolated injury due to the position of the pancreas.
* The most commonly injured intra-abdominal organ in paediatric trauma is the spleen. The liver is the second most commonly injured. Handlebar injuries should raise suspicion for pancreatic injury or pancreatitis in children.
* Amylase elevation will often not occur until 3-4 hours after injury, if at all, and lipase is no more specific for pancreatic trauma.

Notes in abdominal trauma
# Flank injuries may produce retroperitoneal injury to the kidneys or bowel without any initial symptoms. Damage to this area should prompt a search for such injuries as damage to the retroperitoneal portion of the bowel will not produce classical signs of peritonism as the leak will be contained.
# Hemodynamically normal patients without signs of peritonitis may undergo a more detailed evaluation to determine the presence of injuries that can cause delayed morbidity and mortality
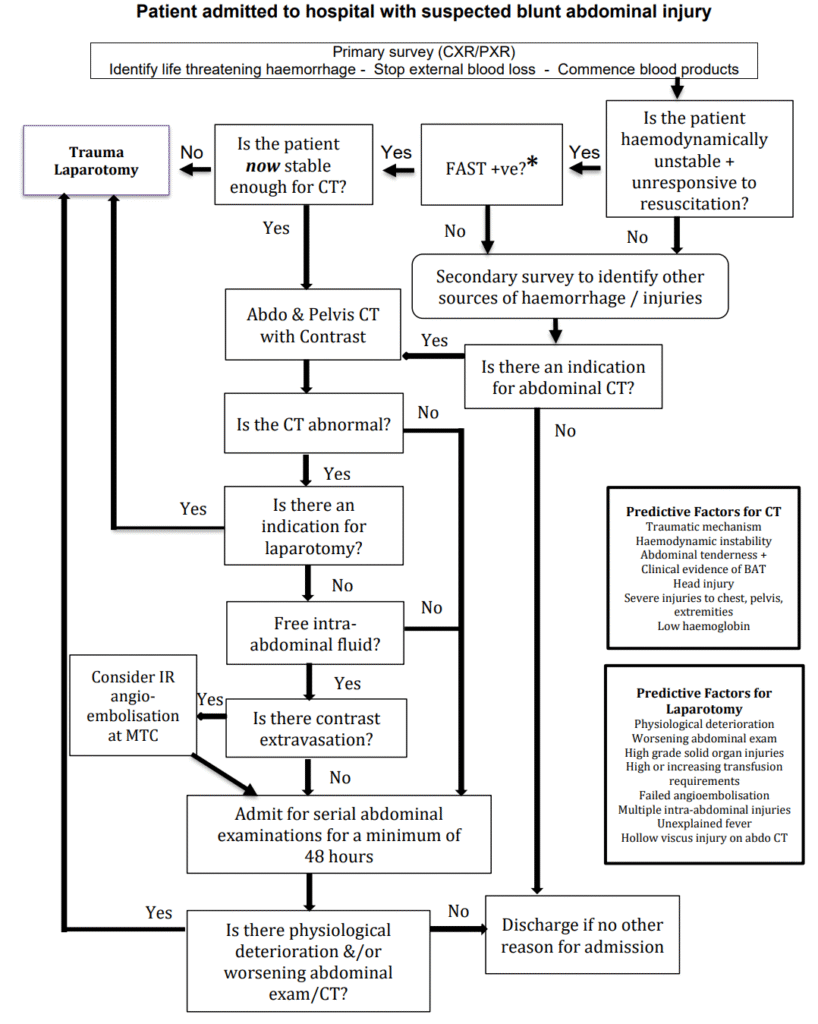
# In patients with hemodynamic abnormalities, rapid exclusion of intra-abdominal haemorrhage is necessary and can be accomplished with either FAST or DPL. The only contraindication to these studies is an existing indication for laparotomy.
# Although a positive FAST may be helpful in this situation, a negative FAST does not exclude the possibility of a visceral injury without a large volume of intra-abdominal fluid
# In the absence of hepatic or splenic injuries, the presence of free fluid in the abdominal cavity suggests an injury to the gastrointestinal tract and/or its mesentery (an indication for early operative intervention).
# Damage to the retroperitoneal portion of the bowel will not produce classical signs of peritonism as the leak will be contained.
# Most abdominal gunshot wounds are managed by exploratory laparotomy.
# Intoxication, head injury or distracting injuries may make clinical assessment of the abdomen unreliable
# An unconscious, anaesthetised or spinally-injured patient will not display signs of guarding
# Intraperitoneal blood will not produce signs of peritonitis
# A high-risk mechanism of injury dictates that a patient should be admitted and re-examined over several hours
# Most commonly injured in gunshot wounds: Small bowel (50%), Colon (40%), Liver (30%) and Abdominal vascular structures (25%)
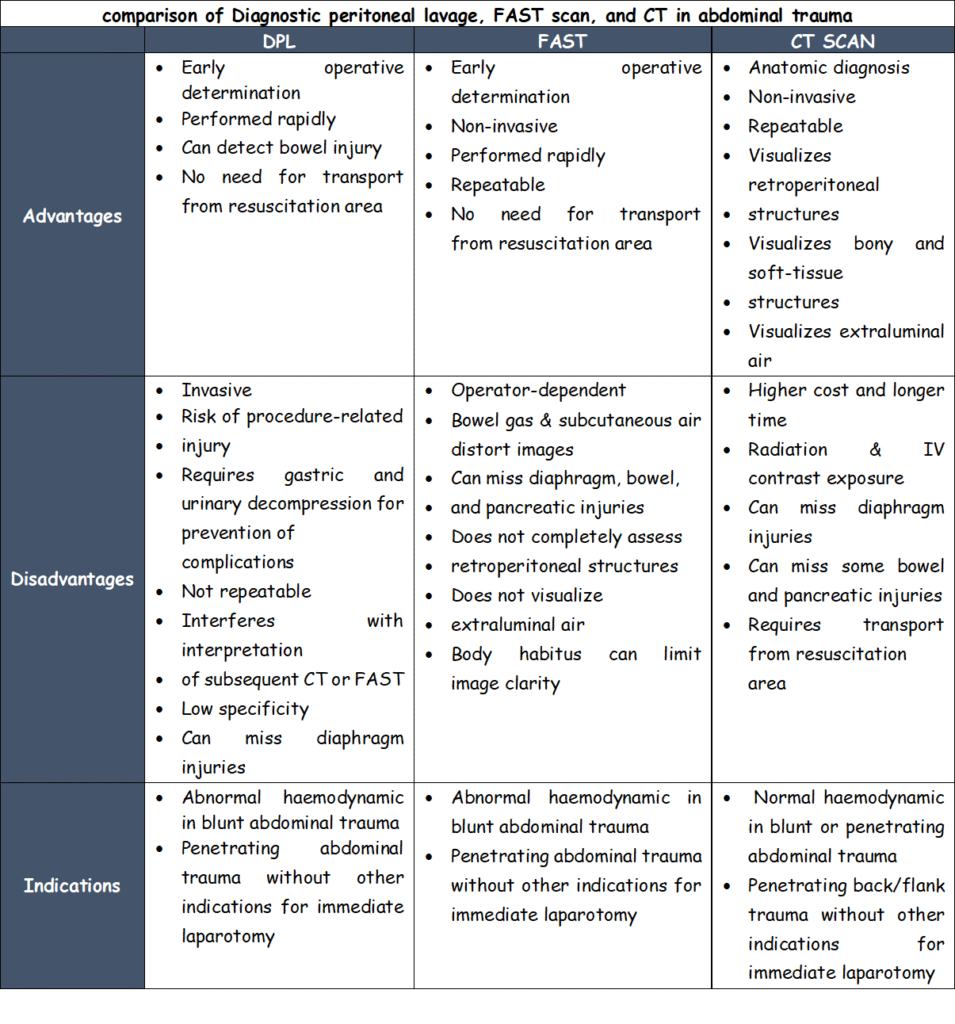
Comparison between DPL / FAST / CT scan