End of life care
What does DNA CPR mean?
- Literally, DNA CPR means do not attempt cardio-pulmonary resuscitation.
- It does not mean we should stop treating the problems likely to cause a cardiac arrest.
- If a DNA CPR is in place, we can still lower the potassium and give the calcium gluconate to stabilise the myocardium. We can still give a fluid bolus, or even some vasopressors. We can give analgesia and anxiolytics. We can even intubate a patient and they can be looked after in intensive care – but if they have a peri-induction cardiac arrest we will not perform CPR.
- In some patients CPR is not appropriate, but ITU might be or ITU might not be. This means many hospitals now have a treatment escalation plan where the “ceiling of care” is discussed, documented and decided. This might be:
- for full treatment, including CPR
- not for CPR, for full active treatment otherwise
- for ward based ceiling of care
- for comfort care
- A DNA CPR is a medical decision, made by the team looking after the patient. The family and the patient should be strongly involved in this decision.
- Learning disability or Down syndrome alone are not reasons to decide against resuscitation.
What is a RESPECT form?
- A RESPECT form is the name given to a form used to document a patient’s wishes.
- It’s not legally binding and can be changed at any time.
- This is the place where conversations between families and Health care physicians can be summarised – dying in hospital or home, religious considerations, music playing etc.
End of life care: –
- As well as asking the asking the patient or their family what their wishes are, we should try and establish if there are any existing decisions or statements of preference about end-of-life care and plan accordingly.
- Any plan made for the patient should document what the goals of care are.
Dealing with end-of-life patient needs the following: –
- Communication is central to ensuring the best possible outcomes.
- Honest communication is crucial in palliative care but is often avoided due to lack of confidence, fear of causing distress, or uncertainty about treatment outcomes.
- Communication goals include informing the patient and their loved ones about likely events, conveying the seriousness of the situation, and exploring the patient’s wishes and priorities.
- Patient Wishes and Advance Care Planning:
- Understanding and Respecting the Patient’s Wishes including Care Planning, CPR Decisions, organ donation
- In the absence of patient communication, family members may provide insights into the patient’s final wishes.
- Lack of capacity requires decisions to be made in the patient’s best interests, guided by family members or loved ones.
- Symptoms management using non-pharmacological and pharmacological methods.
- Continuing care by stopping all non-essential medication, blood tests.
- Providing spiritual support: – Sensitivity to the patient’s faith or community is crucial, and chaplaincy support can be offered.
- Emotional support is essential both for patients and their families.
- Bereavement meetings are offered by many EDs, where families are invited to return to meet senior clinicians as an opportunity to ask questions or seek clarification on events.
Signs that may suggest a person is entering the last days of life such as
- agitation, Cheyne–Stokes breathing, deterioration in level of consciousness, mottled skin, noisy respiratory secretions and progressive weight loss
- functional observations such as changes in communication, deteriorating mobility or performance status, or social withdrawal.
Non-pharmacological techniques for symptom management: –
- Breathlessness: The feeling of air moving over their face can provide great relief, so opening a window or introducing a fan to the room can be refreshing. Fans, however, should be avoided in infectious diseases, such as Covid-19, because of the risk of dispersing infectious droplets.
- Acute Haemorrhage: Using dark coloured towels to absorb the blood can reduce the visual and psychological impact on the patient and any family present.
- Agitation: Nurse in a calm, quiet, low stimulation environment. Look for and address causes of pain or distress, such as a full bladder, full rectum or wet bed. Playing someone’s favourite music through a relative’s smart phone can have a soothing and calming effect.
- Respiratory Secretions: Repositioning may settle the noise of uncleared secretions as can gentle suction to the oropharynx. Secretions are rarely troublesome to the patient themselves; simple reassurance can go a long way in alleviating the family’s distress.
- Pain: Explanations to facilitate understanding of the nature of the pain and the nature and expectations of treatment often allow patients to cope better. Covering open wounds or sores can provide relief, as does splinting fractures.
- Ensure that hydration is maintained in the last days of life when needed, to prevent or minimise unwanted symptoms such as dehydration or delirium.
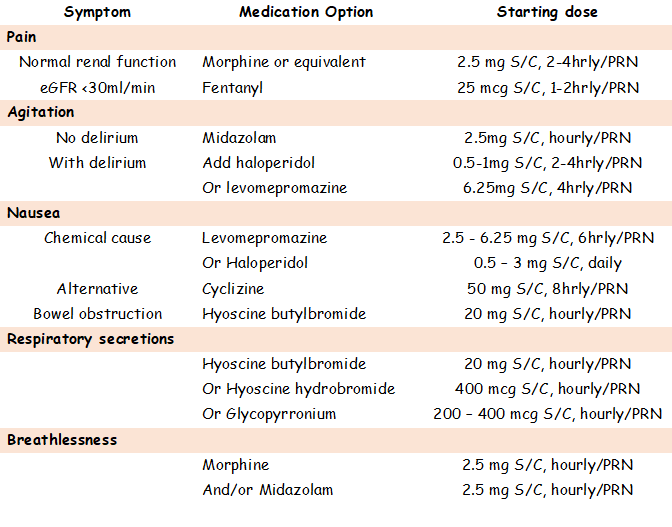
Pharmacological therapies:
Use an individualised approach to prescribing anticipatory medicines for people who will need symptom control in the last days of life. Specify the indications for use & the dosage of any medicines prescribed.
For people in the last days of life with obstructive bowel who have nausea/vomiting, consider:
- Hyoscine butylbromide as the first-line pharmacological treatment
- Octreotide if the symptoms do not improve within 24 hours of starting treatment with hyoscine.
Managing breathlessness: –
- Identify & treat reversible causes of breathlessness, ex. pulmonary oedema or pleural effusion.
- Only offer oxygen therapy to people known or clinically suspected to have symptomatic hypoxaemia.
- Consider managing breathlessness with an opioid (Morphine 2mg s/c, hourly PRN) or a benzodiazepine or a combination.
Managing pain
- Treat any reversible causes of pain, such as urinary retention.
- Morphine 2mg s/c, hourly PRN – for pain and / or breathlessness
- Follow the principles of pain management used at other times when caring for people in end of life.
Managing noisy respiratory secretions
- Consider non-pharmacological measures to manage noisy respiratory or pharyngeal secretions
- Consider a trial of medicine to treat noisy respiratory secretions if they are causing distress to the dying person:
- RCEM guidelines: – Hyoscine Butylbromide 20 mg s/c, maximum of 6 doses in 24hrs
- Atropine or glycopyrronium bromide or hyoscine butylbromide
- Monitor for improvements, preferably every 4 hours, but at least every 12 hours.
- Monitor regularly for side effects, particularly delirium, agitation or excessive sedation when using atropine or hyoscine hydrobromide.
For people in the last days of life who have nausea, consider:
- Levomepromazine 2.5 mg s/c, 8 hourly PRN
Managing anxiety, delirium and agitation
- Treat any reversible causes of agitation, anxiety or delirium.
- Consider a trial of a benzodiazepine – Midazolam 2mg s/c, hourly PRN to manage anxiety or agitation.
- Consider a trial of an antipsychotic medicine to manage delirium or agitation.
- Seek specialist advice if the diagnosis of agitation or delirium is uncertain or if the agitation or delirium does not respond to antipsychotic treatment.