Fever in children (Fever in under 5s)
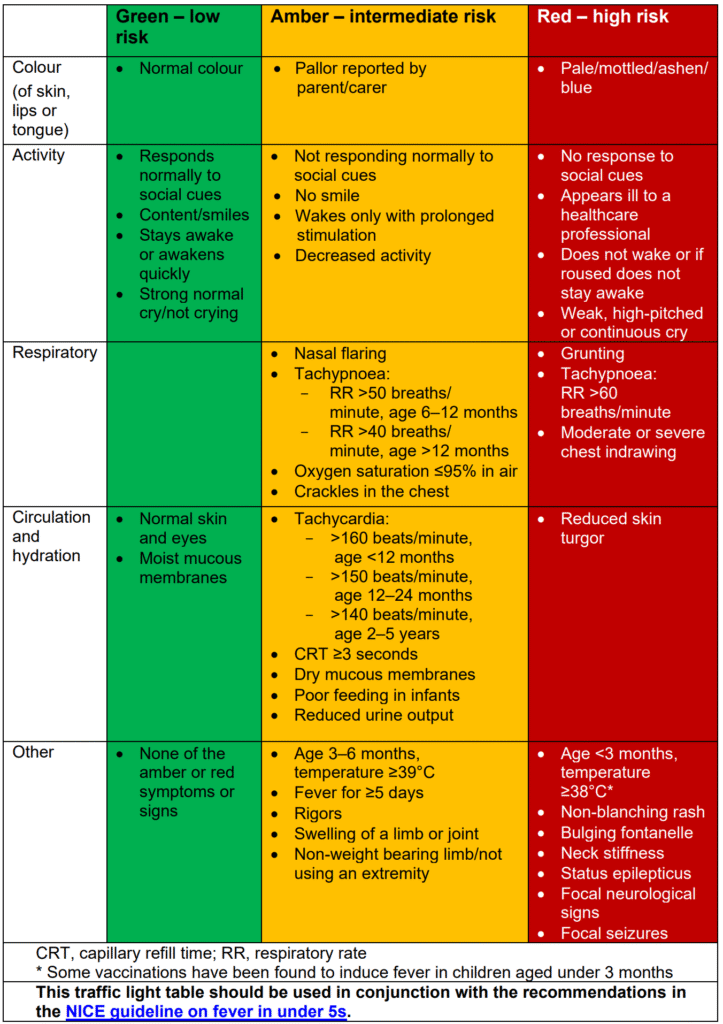
Use a Traffic light system for identifying the risk of serious illness in those under 5s. if a child presents with fever and symptoms or signs that indicate possible sepsis.
| Infants < 3 months with sepsis | Children aged ≥ 3 months with ≥ 1 red feature | Children aged ≥ 3 months with ≥ 1 amber feature |
|---|---|---|
| Measure & record the vital signs (HR, RR, T) Perform the following investigations * FBC, CRP, Blood culture * Urine test if UTI symptoms are present * CXR if respiratory signs are present * Stool culture, if diarrhoea is present Perform lumbar puncture in the following children with fever (unless contraindicated): 1- infants younger than 1 month 2- all infants aged 1 – 3 months who appear unwell 3- infants aged 1 – 3 months with a WBC < 5 × 109/L or > 15 × 109/L. | Perform the following investigations FBC, CRP, Blood culture, urine test if no apparent source. The following tests should also be considered in children with ’red’ features, as guided by the clinical assessment: 1- lumbar puncture in children of all ages (if not contraindicated) 2- Chest X-ray irrespective of body temperature and WBC 3- Serum electrolytes and blood gas. | They should have the following investigations (performed unless deemed unnecessary by an experienced paediatrician). 1- urine test for urinary tract infection 2- blood tests: FBC, CRP and blood cultures 3- lumbar puncture should be considered for children younger than 1 year 4- CXR in a child with a fever > 39°C and WBC > 20 × 109/litre. |
There are instances, however, in which blood tests are beneficial – principally FBC, CRP, blood culture and lactate are indicated in the following febrile circumstances:
- Infant under 3 months of age: due to maternal immunoglobulin cover and their own immature immune system, presentation with fever is more suspicious of bacterial sepsis (You will find in most places, that a child < 3 months with a fever will have a full septic screen)
- Any suspicion of meningococcal infection or meningitis: petechial/ purpuric rash, fever, irritability/lethargy, photophobia, bulging fontanelle… any of these should raise your suspicions, but meningitis should be considered as a ‘rule-out’ differential for all. Remember to take a clotting sample!
- Suspected PUO
- Any child over 3 months of age with a fever of unknown source and 1 or more amber or red feature(s) from the traffic light table
- Consider U&E/LFTs if any concerns about end-organ damage or if the kidneys/liver are the suspected source of fever.
UTI in Paediatrics: –
| Dipstick testing for leukocyte and nitrite is diagnostically as useful as microscopy and culture | |
| If both leukocyte and nitrite are positive | The child should be regarded as having UTI and antibiotic treatment should be started. |
| If leukocyte is negative and nitrite is positive | Antibiotic treatment should be started if the urine test was carried out on a fresh sample of urine. A urine sample should be sent for culture. |
| If leukocyte is positive and nitrite is negative | A urine sample should be sent for microscopy & culture. Antibiotic treatment for UTI should not be started unless there is good clinical evidence of UTI |
| If both leukocyte and nitrite are negative | The child should not be regarded as having UTI. Antibiotic treatment for UTI should not be started, and a urine sample should not be sent for culture. Other causes of illness should be explored. |
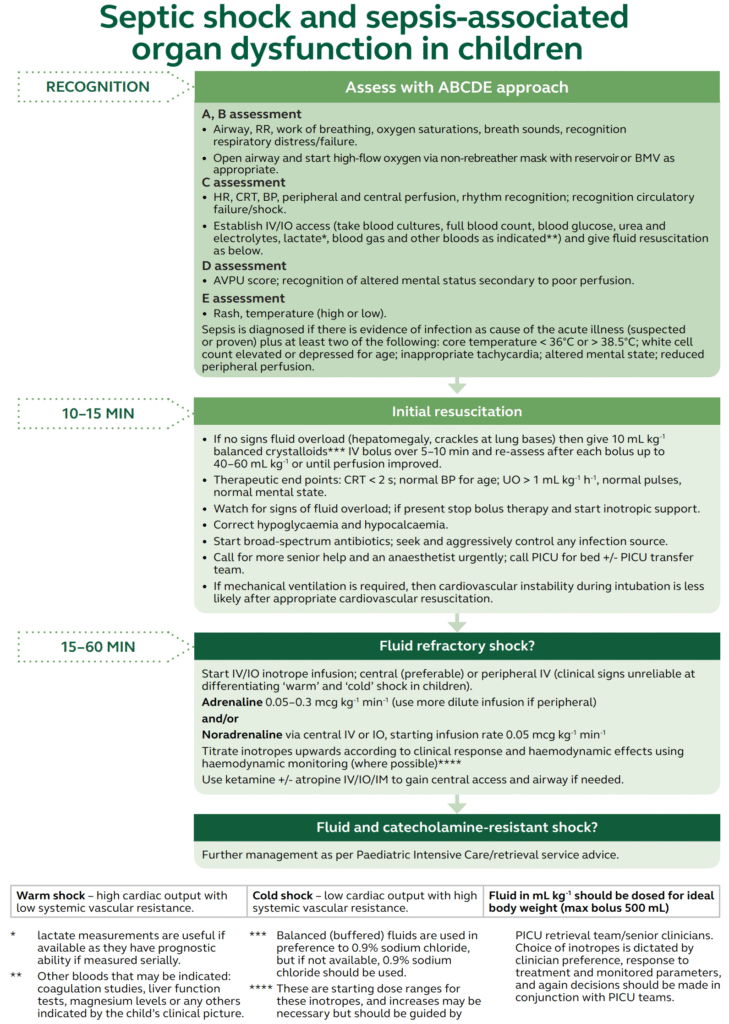
Septic shock and sepsis-associated organ dysfunction in children