Knee & leg injuries
Examination
- Ask the patient to straight leg raise: The ability to do this against resistance virtually excludes quadriceps, patellar tendon rupture, or transverse patellar fractures. If unable (possibly due to pain), ask the patient to kick forwards whilst sitting with the affected leg dangling free.
- Assess the cruciate ligaments using the drawer test:
- Anterior glide (draw) of the tibia (indicating rupture of the anterior cruciate ligament) or
- Posterior glide (draw) of the tibia (indicating rupture of the posterior cruciate ligament).
- Assess the collateral ligaments: With Valgus and Varus Stress Test for medial and lateral collateral ligaments
X-rays for knee injuries
Use the Ottawa knee rules: – X-rays are only required if any of the following are present:
- There is isolated bony tenderness of the patella.
- There is bony tenderness over the fibula head.
- The patient cannot flex the knee to 90⁰.
- The patient could not weight-bear (take at least 4 steps) both immediately after the injury and at the time of examination.
Adopt a lower threshold for obtaining X-rays in those: –
- Aged <18 Or > 55 years
- Patients intoxicated with alcohol.
- Those suffering from bone disease (e.g., RA, documented osteoporosis)
- Those who re-attend the ED with the same injury (having not been X-rayed initially).
Patellar fracture
| Vertical fractures | Transverse fractures |
| Treat with analgesia, immobilize in cricket splint (or non-weight bearing cylinder POP), supply crutches, and arrange orthopaedic follow-up. | unstable due to the pull of quadriceps. Treat with analgesia, immobilization in cricket splint (or a POP back-slab), and orthopaedic referral for probable ORIF |
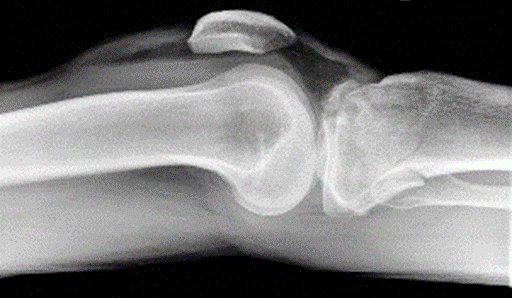
Dislocation of the patella
The patella typically dislocates laterally. Due to twisting motion with flexed knee and internally rotated femur on fixed foot (valgus – flexion – external rotation)
Reduction can usually be achieved using Entonox® à Using a thumb, push the patella medially in one smooth, firm movement whilst gently extending the knee at the same time.
Obtain X-rays after reduction. X-rays are not generally required prior to reduction of the dislocation.
Immobilize in cricket splint or POP cylinder cast, provide analgesia and arrange orthopaedic follow-up in fracture clinic.
Surgery is not usually indicated for first time dislocations.
Tibial plateau fractures
Falls onto an extended leg can cause compression fractures of the proximal tibia.
Valgus stresses crush or fracture the lateral tibial plateau. These injuries are commonly seen in pedestrians injured following impact with car bumpers.
Varus injuries result in crushing or fracture of the medial tibial plateau and are usually associated with rupture of the opposite collateral ligaments.
Look carefully on X-rays for
- Breaks in the articular surfaces of the proximal tibia, avulsions from the ligamentous attachments or loss of height from the medial and lateral tibial plateaux.
- Lipo-hemarthrosis: it results from an intra-articular fracture with escape of fat and blood from the bone marrow into the joint, and is most frequently seen in the knee, associated with a tibial plateau fracture (most commonly) or distal femoral fracture.
Treat with
- Adequate analgesia, immobilization in a long leg POP back-slab and orthopaedic referral.
- Fractures of the tibial plateau often require elevation ± ORIF with bone grafting.
- Admit all patients with an acute hemarthrosis.
- Treat small, isolated avulsions without hemarthrosis with immobilization, crutches, analgesia, and arrange orthopaedic follow-up.
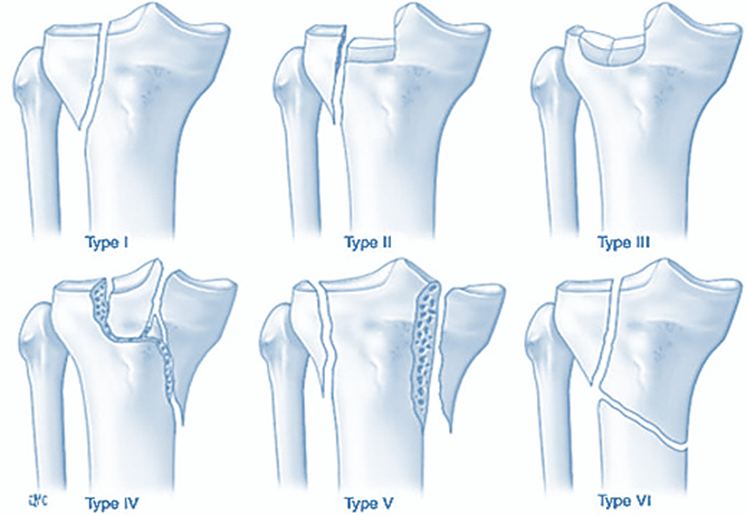
Schatzker Classification for tibial plateau fracture
- Type I – lateral plateau fracture without depression
- Type II – lateral plateau fracture with depression
- Type III – compression fracture of the lateral (type IIIA) or central (type IIIB) plateau,
- Type IV – medial plateau fracture
- Type V – bicondylar plateau fracture
- Type VI – plateau fracture with diaphyseal discontinuity
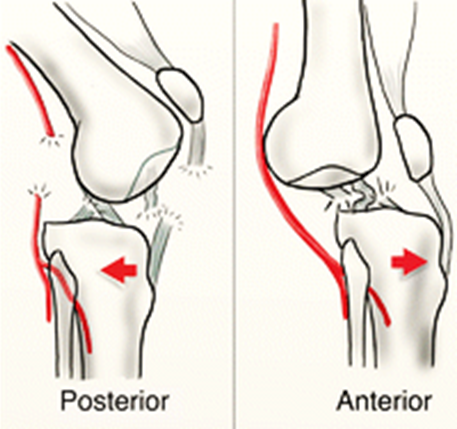
Knee dislocation
Knee Dislocation — It could be medial / lateral / rotatory / anterior or posterior dislocation.
Management: “immediate reduction of obvious dislocation”
- Check and document neurovascular status.
- Evaluate signs of posterolateral dislocation (Dimple Sign) as it is irreducible & any trial of closed reduction leads to skin compression and skin necrosis.
- Reduction – using Entonox® +/- IV analgesia by applying longitudinal traction to the extremity.
- After reduction: immobilise in long leg posterior splint with knee flexion in 15 – 20°
Complications: –
- Popliteal artery injury
- Compartment syndrome of leg
- Common peroneal nerve injury (drop foot)
- Associated fractures or ligamentous injury
Anterior knee dislocation is more common & caused by knee hyperextension. But posterior dislocation carries more risk for popliteal artery injury and caused by direct blow to the proximal tibia displacing it posteriorly.

Tibial fracture
Complications of tibial fractures: acute compartment syndrome, neurovascular injuries, Fat emboli and infection.
Treatment of tibial fractures: immobilization in a long leg POP back-slab, leg elevation and analgesics. Orthopaedic referral for definitive treatment

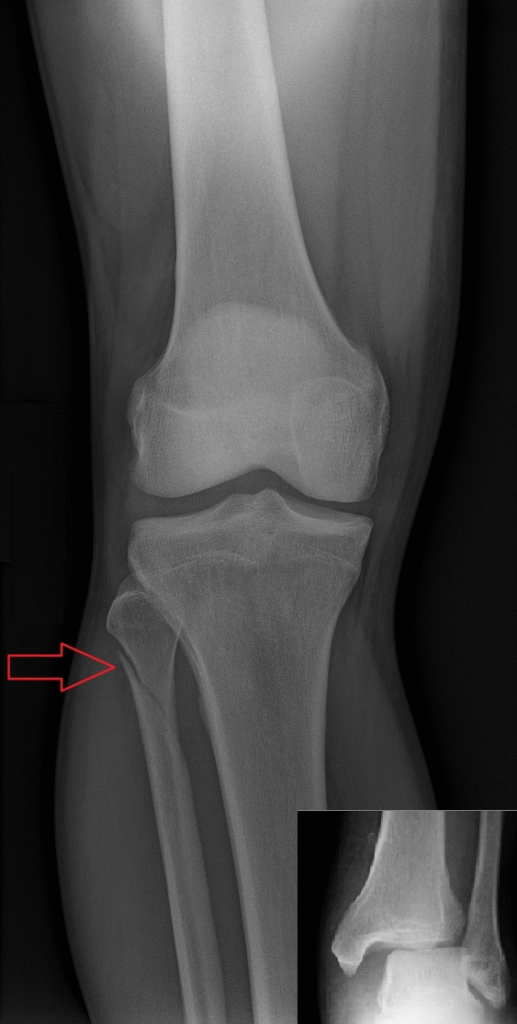
Maisonneuve fracture
- It is fracture of the proximal fibula and damage to the distal tibiofibular syndesmosis and/or deltoid ligament or fracture of the medial malleolus. (Examine the proximal fibula in all ankle injuries and X-ray if locally tender)
- It is caused by external-rotation mechanism.
- It requires surgical fixation
- The common peroneal nerve may be damaged in proximal fibular injuries.
- Examine specifically for weakness of ankle dorsiflexion (drop foot) and decrease sensation of the lateral aspect of the forefoot.
Osgood-Schlatter disease
- It is an apophysitis of the tibial tuberosity that causes anterior knee pain during adolescence and is usually self-limiting.
- The typical age of onset in females may be slightly earlier (boys 10-15 years; girls 8-12 years)
- Pain is: –
- Localized to the tibial tuberosity.
- Gradual in onset and initially mild and intermittent, but may progress to become severe and continuous.

Soft tissue injuries
Ruptured quadriceps
Examination reveals complete inability to straight leg raise. There may be a palpable defect in the muscle insertion. Refer to the orthopaedic surgeon for repair.
Ruptured patellar tendon
Examination reveals complete inability to straight leg raise, a high-riding patella, a palpable defect in the patellar tendon. There is frequently an associated avulsion of the tibial tuberosity. Refer to orthopaedics for repair.
Acutely locked knee
A springy block of the knee to full extension indicates an underlying meniscal injury or other loose body in the knee joint. Obtain knee X-rays (including a tunnel view).
Give analgesia and refer for arthroscopy. Do not attempt to unlock the knee as this is usually painful & futile.
Collateral ligament injuries
Major laxity (i.e., the joint opening up > 1cm) with no end-point implies complete rupture.
Consider cricket splint, and provide crutches, analgesia, quadriceps exercises, and orthopaedic follow-up.
Posterior Cruciate ligament rupture
In posterior cruciate ligament tears, the tibia may appear to sag back when the knee is flexed, so the tibia can be pulled into a more normal position causing a ‘false positive’ anterior draw.
X-rays may reveal the relevant posterior tibial spine to be avulsed. Provide analgesia and refer.
Anterior Cruciate ligament rupture
ACL tears often occur in association with tears of the medial collateral ligament and/or medial meniscus.
Pain & swelling with a history of an audible ‘pop’ at the time of injury.
Radiological finding in anterior cruciate ligament tear
- Deep lateral sulcus sign
- Anterior tibial translocation sign
- Joint effusion
- Segond or Arcuate fracture
- Segond fracture: It is avulsion fracture of the knee that involves the lateral aspect of the tibial plateau and associated with ACL tear. Patient needs MRI and orthopaedic review
Treatment of large traumatic knee effusion: – Aspirate under full aseptic conditions the immobilize in POP knee back-slab or cricket splint and arrange orthopaedic referral.
Calf muscle tears “Acute tears of the gastrocnemius muscle”
It often occurs during sports but it can occur from stepping from a bus or kerb, or from a sudden jump.
Characterised by Sharp or burning pain in the calf is followed by ↑ stiffness or pain on weight-bearing.
Differential diagnosis includes DVT or rupture of a Baker’s cyst. Ultrasound can help to confirm the diagnosis.
Examine for
- Localized tenderness and/or swelling over the calf muscle bellies.
- The medial head of gastrocnemius is more commonly injured.
- Carefully check the Achilles tendon for signs of rupture.
Treat with
- Analgesia, leg elevation and initial ice application. Use of crutches if symptoms are severe.
- Advise progressive weight-bearing as tolerated, arrange follow-up and early physiotherapy if needed.
Management of Pre-tibial lacerations
Use steri-strips instead of stitches then bandage applied from toes to knee. (To ensure that the cut will heal as quickly as possible it is important to maintain a good blood supply to the wound and prevent swelling).
Analgesia and elevation to prevent haematoma formation.
Plastic review may be needed for lacerations with large flap.
