Chest Trauma
Tension pneumothorax
It leads to a shift of mediastinal contents in the opposite direction. Furthermore, a patient who presents as hemodynamically unstable may a pneumothorax with underlying tension aetiology due to various traumatic mechanisms. The circulatory consequences of this kind of anatomical movement can have devastating outcomes when not managed quickly and appropriately.
Clinical features: –
- For awake patients:
- Chest pain and respiratory compromise.
- Decrease SpO2 (early feature); hypotension (late).
- Lateralising sign: decrease breath sounds on the affected side
- Hyper-resonance and tracheal deviation are soft and difficult to elicit.
- For ventilated patients
- Early reliable signs: decrease SpO2 & BP associated with Tachycardia
- Sudden rise in ventilation pressure > 40 mmH2O
- Lateralising signs are the same as for awake patients.
@ If your patient is not critical then request an urgent resus room CXR. In critical patient diagnosis is clinically
@ The eFAST and/or portable CXR may help in your assessment of tension pneumothorax, unless the patient is critical. Radiological evidence of tensioning does not necessarily correlate clinically.
@ One third of initial CXRs in trauma will not detect pneumothorax anaesthetic colleagues need to be aware of this if your patient leaves for theatre.
@ Cardiac tamponade may give similar signs clinically shock, with distended neck veins. A combination of your FAST skills, urgent CXR and consideration of the mechanism of injury should help you distinguish the two.
@ Beware other pathology masquerading as large (possibly tensioning?) pneumothorax on the CXR, for example an emphysematous bulla or Gastrothorax.



thoracic_trauma_lge_1-300×266.jpg (300×266) (rcemlearning.co.uk)
{kind=link}
thoracic_trauma_lge_4-300×245.jpg (300×245) (rcemlearning.co.uk)
{kind=link}
thoracic_trauma_lge_5-249×300.jpg (249×300) (rcemlearning.co.uk)
{kind=link}
Treatment: –
| Treat Tension Pneumothorax in Peri-arrest / Arrest by Thoracostomy followed by chest drain |
| Treat Tension Pneumothorax in stable patient by Needle thoracocentesis followed by chest drain |
* The current ATLS guidelines recommend needle decompression (14-gauge cannula) via the 4th or 5th intercostal space anterior to the mid-axillary line in adult. (2nd intercostal space in child)
* If there is good clinical and radiological evidence of significant lateral chest wall injury – consider the chest drain insertion in the 2nd intercostal space anteriorly.
* Gross surgical emphysema in combination with pneumomediastinum and a chest drain that continues to bubble, suggests tracheo-bronchial injury. Consider insertion 2 x wide bore chest drain, one space between them, and do not attach suction to the chest drain.
* Confirm that the drain lies within the chest wall cavity by looking for fogging of the tube and swinging of the chest drain with respiration.
Open pneumothorax
(Known as communicating pneumothorax or sucking chest wound)
A hole of only 1 or 2 cm in radius may cause serious respiratory compromise, particularly in patients with comorbidities, and/or other injuries
Treatment: –
- Definitive treatment is surgical repair.
- if not already done so by the paramedics: –
- Cover the wound, with specific chest seal devices.
- Cover the wound with 3-side sterile occlusive dressing, if chest seal device is not available.
- If the hole is too big, cover with a large Opsite, make a small hole in the middle and place a chest seal device on top if available.
- Early intubation: IPPV solves the respiratory embarrassment created by the hole in the chest.
- For small open pneumothoraces, insert a chest drain remote from the wound on that side.
- Do not insert a chest drain in patients with a large open pneumothorax since muscle flaps may be needed for closure and can be damaged in the procedure.
Massive haemothorax
Massive haemothorax is defined by the need for thoracotomy — the indications are:
- Blood loss > 1,500 mL or 1/3rd of blood volume
- Blood loss >200 mL/h (3 mL/kg/h) for 2-4 hours
- Continued need for blood transfusion
It creates a problem because of shock (haemorrhagic and impaired venous return from the vena cava) and decreased ventilation (the lung on that side gets compressed).
Haemothorax is most commonly caused by haemorrhage from intercostal or internal mammary arteries secondary to blunt and penetrating trauma.
Use CXR and FAST to guide you. You may underestimate the size of the haemothorax on a supine CXR. Ultrasound has greater sensitivity than supine chest radiography in detection of haemothoraces.
Treatment: –
Should be focused on simultaneously 1) restoring blood volume while also 2) decompressing the chest
– Use blood & blood products early, with activation of major haemorrhage protocol if necessary.
– A 28 – 32 F chest tube should be placed to decompress the chest and improve ventilation.
– Ideally connect the drain to a cell salvage/saver machine (auto-transfusion), fill the underwater seal with saline as the saline/blood collection can still be run through a cell saver later.
- When > 1500 ml of blood immediately returning from the chest tube, this is an indication for an urgent thoracotomy. Involve your cardiothoracic surgeons early in the care of these patients.
– Occasionally a massive haemothorax may be well tolerated, typically in young patients with a chest stabbing. Delaying chest drain insertion until reaching thoracic theatre, where cell salvage exists, is an option depending on availability of skills and theatre space.
Cardiac tamponade
With a penetrating injury to chest, back or upper abdomen – think tension pneumothorax, massive haemothorax, and cardiac tamponade. Exclude or confirm tamponade with a FAST scan.
50 – 200 ml of blood in the pericardial sac may be enough to rapidly cause PEA cardiac arrest.
The classical clinical signs: “Beck’s Triad”
- Distended Neck veins (may not be distended if the patient has haemorrhagic shock)
- Hypotension (and a raised respiratory rate)
- Muffled heart sounds (difficult to be heard in the ED)
Treatment: –
- ABCD approach and Fluid resuscitation to increase pre-load
- If the patient is haemodynamically stable refer for urgent surgical exploration in theatre. Look for co-existing injuries (especially pneumothorax) on a portable CXR first
- Thoracotomy if the patient presents within 10 minutes of cardiac arrest
ATLS advises pericardiocentesis only as a temporising measure, pending thoracotomy if not available.
Flail chest
This occurs when 3 or more ribs are fractured segmentally (i.e., in more than one place) resulting in a free or floating section of the chest wall.
A CXR might identify associated pneumothorax, haemothorax and pulmonary contusions. The appearance of early pulmonary contusions is particularly worrying, and evidence of further and perhaps more extensive contusions with physiological effect may evolve.
Beware and don’t forget: –
- underlying pulmonary contusions which may cause significant morbidity and mortality in any age group.
- Considerable force is required to create a flail chest in young people look carefully for other injuries, both intra and extra-thoracic
- Multiple rib fractures are a potential source of significant haemorrhage.
Treatment: –
- Start in ABCD approach
- For patients with major trauma
- Proceed to intubation & ventilation (IPPV). (to control of respiratory compromise)
- Analgesics (remember to give adequate morphine post RSI)
- Insert a chest drain for associated pneumothorax and haemothorax.
- Judicious fluid resuscitation since excessive fluid floods injured lung tissue.
- Early referral to cardiothoracic surgeons for definitive surgery (internal fixation of ribs)
- If there are no other life-threatening injuries: – Discuss conservative treatment options with ICU and cardiothoracic surgeon which may include the use of thoracic epidural, intercostal nerve blocks or patient-controlled analgesia, and CPAP and physiotherapy.
Pulmonary contusion
Look for patchy white areas progressing to frank consolidation on the CXR (aspiration and haemorrhage are differential diagnoses)
If lung Contusions are visible on the initial CXR, suggest significant injury. Deterioration with abnormal blood gas derangement likely to follow.
Computed tomography (CT) imaging is more sensitive for the detection of pulmonary contusions. A lung consolidation within 6 hours of blunt trauma lasting 48 to 72 hours is diagnostic for a pulmonary contusion.
Look for associated rib fractures and haemo/pneumothorax. Rib fractures do not always co-exist, particularly in the young, where their existence indicates that significant force created the injury.
They are potentially life threatening as:
- The patient is at risk of hypoxaemia
- Because of the force involved to cause the injury, associated injuries are common
- Injured lung is vulnerable to flooding from aggressive fluid resuscitation.
Treatment: –
- IPPV with Positive End Expiratory Pressure (PEEP) for the sicker patients. follow “Good Lung Down” protocol to improve ventilation-perfusion matching.
- Judicious use of fluids. Consider insertion of a central line and arterial line
- Discuss patient’s condition with ITU and thoracic surgical colleagues
- No evidence for steroids or prophylactics antibiotics
- Avoid colloids since these will breach injured lung tissue and worsen hypoxia
Myocardial contusion
Myocardial bruising caused by blunt injury, including deceleration and ballistic mechanisms.
Clinical assessment and identification
- A normal ECG effectively rules out the condition.
- Unexplained tachycardia may be a clue. Look too for atrial & ventricular ectopics.
- Consider bedside echocardiogram and troponin
Treatment: –
- Monitor ECG.
- Consider a central and arterial line.
- Treat the following if identified: Hypoxaemia / Acidaemia / Fluid status / Low haemoglobin
Aortic injury
Several CXR features might suggest the injury according to ATLS:
- Widened mediastinum the most reliable sign
- Fractures of the first and second ribs
- Obliteration of the aortic knob
- Deviation of the trachea to the right
- Presence of a pleural cap
- Elevation & rightward shift of the right main stem bronchus
- Depression of the left main stem bronchus
- Obliteration of the space between the pulmonary artery and the aorta
- Deviation of the nasogastric tube to the right
Contrast CT thorax is the investigation of choice.
Mediastinal haematoma can be caused by Aortic injury or sternal fracture or thoracic vertebral fracture.
Treatment: –
- Control hypertension (SBP < 110 mmHg) & tachycardia with appropriate analgesia and labetalol.
- Surgical repair or endovascular stenting
Diaphragmatic injury
Diaphragmatic injury is usually caused by penetrating rather than blunt injury.
In blunt injury, it is 3 times more common on the left (the right hemi-diaphragm protected by the liver) and nearly always at the weakest point, postero-laterally.
Examine the CT carefully in patients who have sustained increase in intra-abdominal pressure.
Treatment: –
- ABCD approach
- Insert a NG tube gently to drain stomach content.
- A cautiously placed a chest drain using the traditional open technique with care to avoid injuring abdominal contents (not Seldinger)
- Surgical repair needs to be considered in the context of associated injuries.
- Diaphragmatic injury needs to be excluded by surgeons in cases of penetrating injury requiring theatre
Posterior Sternoclavicular Joint Dislocation
It is clinically important since the medial clavicular head may compromise the airway or major vessels.
If there is evidence of compromise, reduction of the dislocation should be attempted.
Abduct the arm to 90 and extend 10 – 15 and apply traction (with counter attraction to the torso from another colleague); maintain traction and pull the medial end of the clavicle forward with your fingers and thumb.
If this fails, prepare the skin with iodine and local anaesthetic and repeat with a towel clip
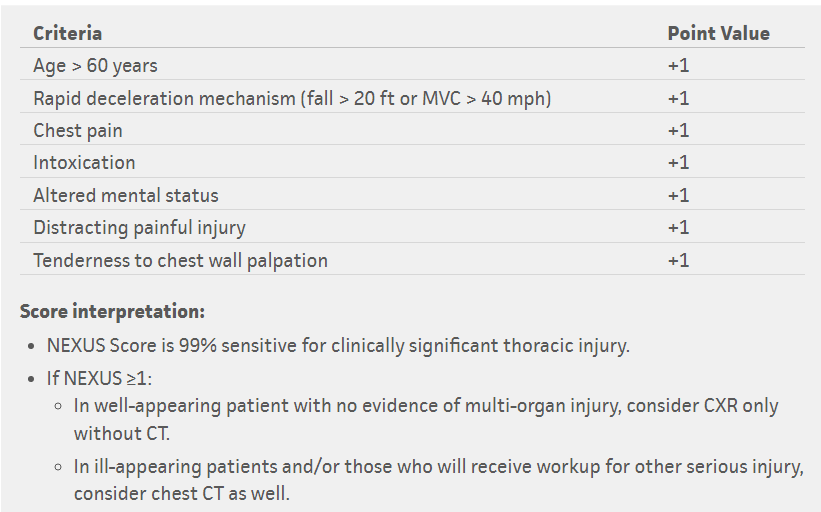
The NEXUS decision instrument: – is applied in a hemodynamically stable adult (older than 14 years) blunt trauma patient when the clinician initially believes chest imaging may be needed. If none of the NEXUS criteria are present, then imaging (CXR and chest CT) can be foregone safely without missing significant injury.