Bowel Obstruction
Adhesions from previous surgery are the leading cause of small bowel obstruction in industrialised countries (70%), followed by malignancy, IBD, and hernias.
Malignancy and volvulus are the commonest causes of large bowel obstruction.
The more proximal the obstruction, the more the fluid loses (third-space losses). As Obstruction → bowel dilatation & abdominal distention → fluid shift out of bowel to the peritoneum +/- perforation → Peritonitis → vascular shift into the peritoneal cavity → hypovolaemia, dehydration and shock.
Clinical features: –
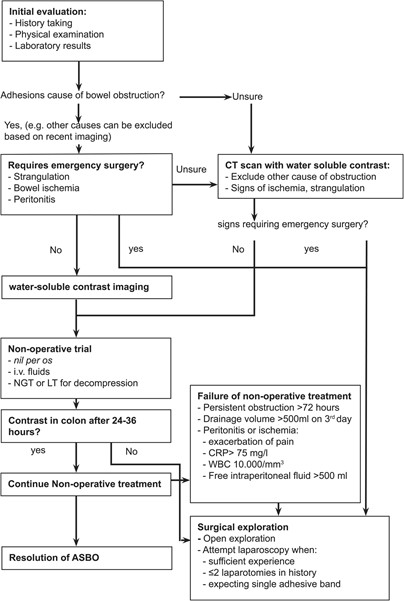
Initial assessment of the patient should involve concomitant history taking with prompt identification of the shocked patient. Generic treatment incorporating analgesia and fluid resuscitation should be performed alongside the initial history and examination.
Constipation and abdominal distension in the patient with a previous history of bowel surgery are strongly suggestive of intestinal obstruction.
Classic symptoms of bowel obstruction: colicky abdominal pain & distension, vomiting and constipation
- Vomiting is a late feature with large bowel obstruction.
- Severe pain in bowel obstruction suggests complications such as ischaemia or perforation
Examination: –
- Rule out other causes of acute abdomen, in particular a ruptured AAA or ectopic pregnancy.
- A rectal examination must also be performed demonstrating an empty rectum or obstructing mass, ideally only once.
- The six variables with highest sensitivity for a diagnosis of bowel obstruction were – a distended abdomen, increased bowel sounds, history of constipation, previous abdominal surgery, age over 50 years and vomiting.
Investigations:
Early CT scan of the abdomen and pelvis with IV contrast helps to identify the level and cause of the obstruction, and therefore determine the management plan.
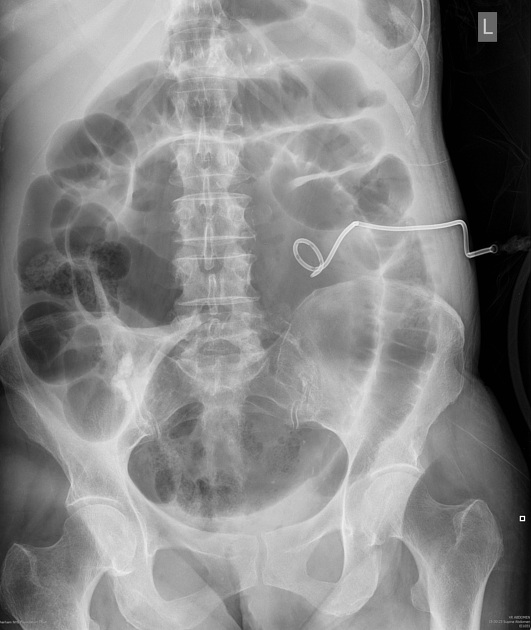
Abdominal X-ray film: consider if there is a delay/unavailability in obtaining abdominal CT scans
- Request Erect chest for free air and supine abdominal X rays.
- The 3/6/9 rule for bowel imaging – upper limit of 3 cm for small bowel loop width, 6 cm for colon and 9 cm for cecum can be used to look for obstruction.
- Small bowel can be differentiated from the colon by the valvulae conniventes, which completely cross the small bowel wall. The taeniae coli of the large bowel are incomplete across the bowel wall.
- The relatively central position of the small bowel and restriction in dilatation to 5 cm also helps to distinguish small from large bowel on plain films.

Radiopaedia.org. From the case rID: 74732

Radiopaedia.org. From the case rID: 150037
Radiopaedia.org. From the case rID: 33334
- Arises in the right lower quadrant
- Extends towards the epigastrium or left upper quadrant
- Colonic haustral pattern is maintained
- Distal colon is usually collapsed and the small bowel is distended

Radiopaedia.org. From the case rID: 10633
- arises in the pelvis (left lower quadrant)
- extends towards the right upper quadrant
- ahaustral in appearance
- Usually has inverted U-shape appearance.
Management: –
- Resuscitate, Treat as mentioned before in acute abdominal pain, and early surgical involvement
- Small bowel obstruction is often treated conservatively, but large bowel obstruction generally requires operative intervention.
- Patients who present with uncomplicated Sigmoid Volvulus (No perforation, No signs of peritonitis) are initially managed by endoscopic decompression either with rigid or flexible sigmoidoscopy, with insertion of a rectal tube for 24 –48h in order to maintain reduction and lessen the risk of early recurrence.
– Hernias –
| Hernia | Anatomy | Incidence |
| Indirect inguinal hernia | Bowel passes through inguinal canal via a congenital weakness of the internal inguinal ring | most common |
| Direct inguinal hernia | Hernia exits abdominal cavity directly through the deep layers of the abdominal wall | uncommon |
| Femoral hernia | Abdominal contents pass through femoral canal just below inguinal ligament | rare |
Strangulation of hernia is a surgical emergency which requires early detection and management to avoid permanent damage. Risk factors: older adult, short duration of hernia, femoral, small diameter
Incarcerated femoral hernias are the most common incarcerated abdominal hernia, with strangulation of a viscus carrying up to 14% mortality.
Functional obstruction results from atony of the intestine and loss of normal peristalsis. Different terms are often used to describe functional obstruction of the small or large bowel: paralytic ileus and pseudo-obstruction respectively.