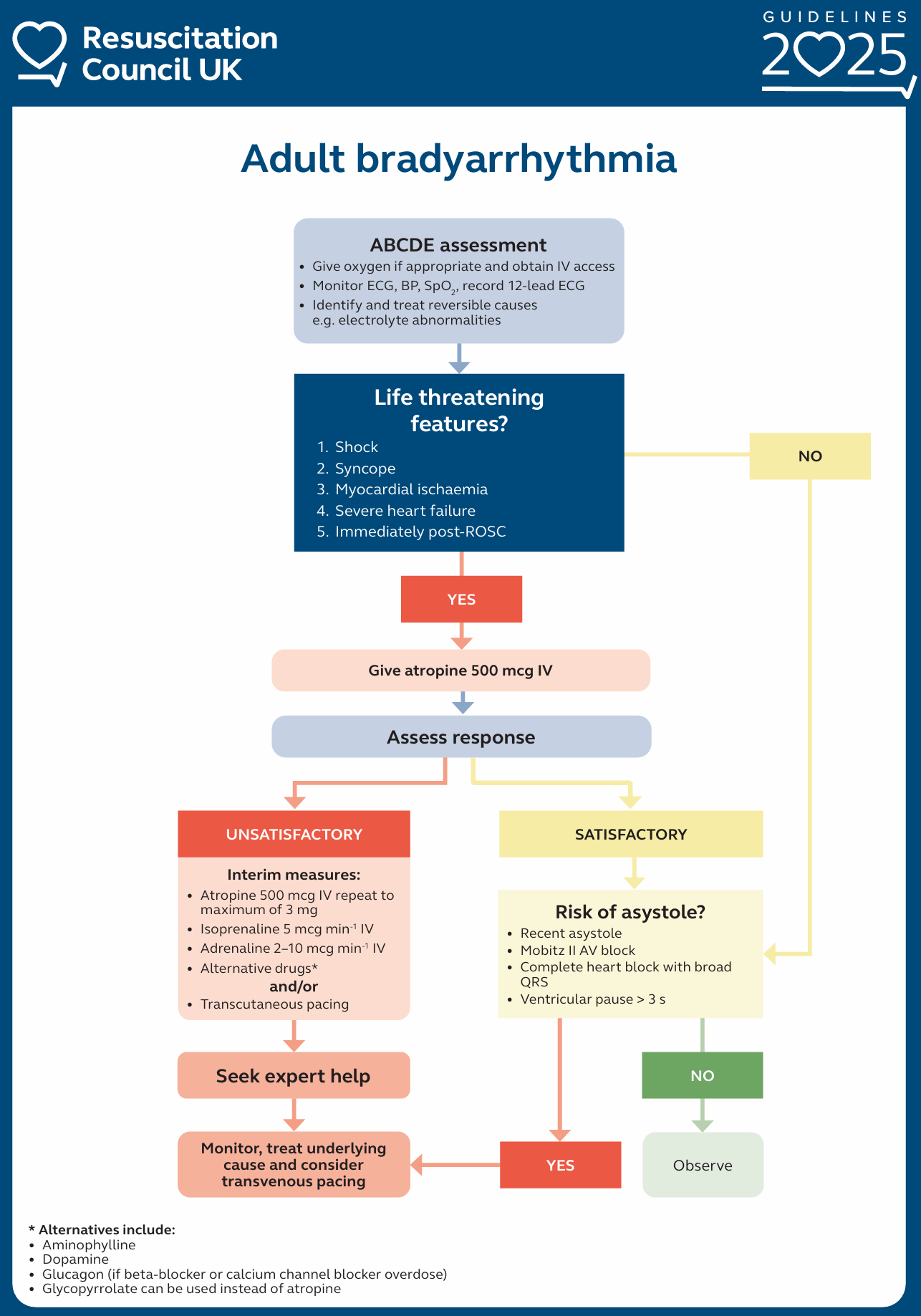
Bradycardia in Adults
If bradycardia is accompanied by life-threatening adverse signs, give atropine 500 mcg IV (IO) and, if necessary, repeat every 3 – 5 minutes to a total of 3 mg.
If treatment with atropine is ineffective, consider 2nd line drugs. These include isoprenaline (5 mcg min−1 starting dose), and adrenaline (2 – 10 mcg min−1).
For bradycardia caused by inferior MI, cardiac transplant or spinal cord injury, consider giving aminophylline (100 – 200 mg slow IV injection).
Consider giving glucagon (2 – 10 mg IV in glucose 5% –then– 50 micrograms/kg/hr IV infusion) if beta-blockers or calcium channel blockers are a potential cause of the bradycardia.
Do not give atropine to patients with cardiac transplants – it can cause a high-degree AV block or even sinus arrest – use aminophylline.
Consider pacing in patients who are unstable, with symptomatic bradycardia refractory to drug therapies.
If transcutaneous pacing is ineffective, consider transvenous pacing.
If atropine is ineffective and transcutaneous pacing is not immediately available, fist pacing can be attempted while waiting for pacing equipment.